At what number can we stop wearing masks, stop social distancing, start dining in, etc.? That's the number I care about. Because until somebody influential picks that number, we'll just keep masking and social distancing until the end of time.
I think we could just stick with positivity rates and case numbers to figure that out, like we have been doing. Once the vaccines start working their magic, we’ll see it in those metrics.
That way we don’t have to try and guess how infectious someone can still be after they have had the vaccine
Exactly. Fixating on the vaccination percentage is simply using a number that's two steps removed from what's actually important.
It's like trying to decide if it's too rainy to go out by figuring out how many people are watering their yards right now, when you could just look out and see if it's raining.
Still we use weather forecast when we decide to make plans tomorrow. The best way to predict wether we can make plans (summer holidays, festivals, etc.) should involve some combination of the vaccination percentage and epidemological models.
Seeing what the case positivity is this week is the best way to decide whether the vaccine has been effective enough to go out this week.
Looking at the vaccine numbers for this week is a worse proxy. How does it help?
Sure, you could use the projected vaccinations for next March to decide how likely it is that you'll be able to go and watch a broadway show in March, but, like the weather forecast, you'll need to know what the actual positivity is in March to make the final decisions.
This is the new “we have no evidence masks help” or “no evidence of asymptomatic spread”.
Name a vaccine that doesn’t reduce onward transmission even as it cures disease. It’s overwhelmingly likely that the vaccine will slow transmission and foolish to throw our priors in the garbage bin.
What we don’t know yet is how much onward transmission will be reduced.
I looked into this, and it does seem the vaccine reduces transmission. It just doesn’t stop it entirely. The paper below is Wikipedia’s source. Upon a close read, in the daycare there were three groups of vaccinated children:
* Those positive for antibodies but pcr negative —> had been exposed, cleared virus without infection
* those pcr positive but asymptomatic
* those pcr positive and symptomatic
About 30% were in the seropositive group which didn’t have pcr positivity. So it seems like transmission was reduced at least 30%. It’s also possible the other two groups would have had lower transmission rates than if they had had no vaccine.
If you have a more precise source I’d be interested to see it, but if this is the worst case it’s pretty good!
> We used PCR, EIA, and culture to confirm B. pertussis infection in two highly vaccinated groups of children in two day-care centers. Three (10%) of 30 2- to 3-year-old children were seropositive for recent infection; one had nasopharyngeal colonization and a clinical illness that met the modified WHO case definition. In the day-care center for the 5- to 6- year-old group, 9 (55%) of 16 children were IgM positive, 4 (25%) of whom had nasopharyngeal colonization. Of these four children, three had nonspecific cough, and only one met the modified WHO definition for pertussis. None of the children in our study, including those who met the WHO definition, had been examined by a physician before our investigation.
>Children who were seropositive and re- mained both asymptomatic and PCR negative probably had sufficient immunity from vaccines or natural boosters to protect them against persistent colonization and clinical disease. Their seropositivity could not be due to vaccine because the children were tested more than a year after having been vaccinated.
> In this paper they've used 45 for HIV. What's your point?
There is a difference between HIV vs SARS-Cov2: If you get AIDS, your body does not have the capacity to recover from it on its own. So, 1) the chances of detecting dead material from a long gone infection are nil; and 2) the cost of a false negative is much higher than the cost of a false positive.
Since most people seem not to be seriously affected by a SARS-Cov2 infection, neither is true for SARS-Cov2. So, not agreeing on a fixed, reasonable, standard number of cycles which everyone uses has the consequence of inflating false positives for no gain. Note WHO's updated information[1].
> WHO guidance Diagnostic testing for SARS-CoV-2 states that careful interpretation of weak positive results is needed (1). The cycle threshold (Ct) needed to detect virus is inversely proportional to the patient’s viral load.
If you are not sick and your viral load is barely detectable, what's the point?
So you think they should use some lower Ct number for which it would be possible to show that eg 99.5% of people who are over it (i.e. have lower viral load) don't infect anyone? Interesting. I've read that most of the false negative for a PCR test actually come from sample collection (makes sense, PCR is super reliable) so it could be that you would miss people with high viral load where the sample was just not taken in a perfect way. Especially early in the infection it could be quite localized.
> So you think they should use some lower Ct number
Everyone should use the same number in all tests. From what I understand, about 20 is a reasonable number which might still result in positives up to a month post-infection. I consider having a standard more important that the specific number chosen. It seems when people go to > 30 it is in a quest to ensure a positive test result.
I fail to see what this has to do with vaccines and infectivity.
Also I’d only heard of people speak in terms of “positive” for pcr. You can be positive but not infectious, if there are a lot of cycles and you’re tested as the disease winds down.
Living in Israel I can tell you that the (current) plan involves masks and distancing for the entirety of 2021. We now have reasonable evidence that those vaccinated folks are still transmitters of the virus, and as of today, the majority of new cases in the last 48 hours were from the UK strain that targets children.
The real worry here is unfortunately human behaviour and not science. The science is clear, and it's been said/written/screamed/spraypainted that the #1 reason we have all of these restrictions is actually human behaviour as opposed to the virus itself.
>The science is clear, and it's been said/written/screamed/spraypainted that the #1 reason we have all of these restrictions is actually human behaviour as opposed to the virus itself.
Nope, if the virus didnt exist, there would be no restrictions; therefore, it is the primary reason.
Has there ever been a control group or any historical precedence to scientifically support the questionable hypothesis that a highly contagious virus can be can be globally controlled simply by controlling human behavior? (i.e. locking down entire nations while "essential workers" -- poor people -- are still forced to go to work)
No evidence that it doesn't, either. It's simply hard to get this evidence and irrelevant for getting vaccines approved, so nobody has bothered. And it'd be really odd if it didn't help wrt infection rate.
Well it's only 40% if you count only the over age 16 population. (Israel is not vaccinating under age 16 until more information.)
If you look at the entire population, it's only about 28% got 1st dose and 12% got second dose, many within the last week.
But with a population of about 9.3 million (size and population comparable to New Jersey) and they just ramped up to about 1million vaccinations a week, we could be at "full" vaccination March 26th - 85% of eligible population, 2nd dose, and 1 week for it to take affect.
> I think we could just stick with positivity rates and case numbers to figure that out, like we have been doing
Sticking only with positivity rates is misleading even if one ignores all the costs of lockdowns. As the WHO pointed out on 13 January 2021[1]:
> WHO reminds IVD users that disease prevalence alters the predictive value of test results; as disease prevalence decreases, the risk of false positive increases (2). This means that the probability that a person who has a positive result (SARS-CoV-2 detected) is truly infected with SARS-CoV-2 decreases as prevalence decreases, irrespective of the claimed specificity.
You may find this comment[2] by me and the link to the calculator to understand the impact of varying prevalence keeping false positive and false negative rates constant.
Note also,
> Most PCR assays are indicated as an aid for diagnosis, therefore, health care providers must consider any result in combination with timing of sampling, specimen type, assay specifics, clinical observations, patient history, confirmed status of any contacts, and epidemiological information.
In plain English, that says that with no illness and no contact with people suffering from Covid19 etc, a positive test does not necessarily mean that the person testing positive is infected.
This is all basic Stats but it has been conspicuously ignored for almost year now.
> The cycle threshold (Ct) needed to detect virus is inversely proportional to the patient’s viral load.
So, before the test, pick a Ct, and stick with it instead of keeping on going until you get a positive result. At higher counts, the test might be detecting left over material from a long gone infection.
> Where test results do not correspond with the clinical presentation, a new specimen should be taken and retested using the same or different NAT technology.
So, if you are sick and get a negative, test again to make sure you can rule out SARS-Cov2. But, equivalently, if you are not sick and test positive, also make sure that this is not a false positive.
The latter is what has been globally ignored with one positive test on healthy people is regarded as proof of infection and illness. It is what is being ignored when people are not allowed to travel or work due to a positive test result. Basically, a positive test result, even without symptoms, and even with a subsequent negative, puts a scarlet letter on you which cannot be erased.
The flowchart in Figure 1 in this document[3] might also be useful. Note the first box is labeled "Patient meets the clinical criteria for COVID-19". That's where these diagnostic tests are applicable as proof of infection.
The fact that the test is useful for confirmation of infection conditional on presenting symptoms doesn't mean it is useful for screening an entire population or deciding on how much GDP to destroy because of the simple facts that in that scenario a large portion of positive test results will be false positives and these tests have high false negative rates.
The concern is that we might end up in the same awkward spot we hit in the summer, where non-conscientious people decide everything's okay and nobody wants to relax the official restrictions for fear of emboldening them. (If you were strictly following California's published rules, for example, you wouldn't have had any private gathering for any reason between March and October.)
At what number can we stop wearing masks, stop social distancing, start dining in, etc.? That's the number I care about. Because until somebody influential picks that number, we'll just keep masking and social distancing until the end of time.
It's not clear yet if arm injected vaccines will provide mucosal immunity. They'll prevent serious disease but epithelial cells in the nose, mouth, and so on can still be infected and shed virus. It's the same for flu vaccines. There are nasal vaccines which do provide mucosal immunity like flumist but during heavy flu seasons only the old and young have access.
So, even if you're the required 2 months post vaccinated you probably shouldn't stop wearing a mask or social distancing until 100% of the population around you has either also been vaccinated or been infected and recovered.
When will the entire population be vaccinated or already infected? At current rates it may be a year or two.
I have been downvoted elsewhere in this thread for saying that it's not clear whether the vaccine confers sterilizing immunity (or perhaps, for suggesting that restrictions will continue until children are vaccinated. Who knows!) Be careful what you say here, lest you get downvoted to oblivion!
When children are vaccinated. It's not clear if the vaccine confers sterilizing immunity, i.e., you are protected against the bug and also can't spread the disease, so most people who have children or are around children will ideally not take undue risks.
I'm not sure if under-16 cohorts' trials are underway already. If they are, and if children are going to be vaccinated before their next school term starts, then society as a whole may consider dropping the current precautions.
First, that’s factually incorrect. Second, children can transmit COVID even if they don’t get severe cases. Ever send a kid to school or daycare and then spend a year or two sick with everything every child in that school or daycare had? Kids spread cold/flu like viruses probably faster than anyone.
That has been true for us up until the pandemic - at least in our case. The combination of the school taking extra precautions and parents not sending sick kids to school is working. We've had our daughter in daycare for months with 1 total illness (minor cold). And in that case I believe it was from taking her to outdoor dining. Kids seem to touch every part of those restaurant high chairs which are never sanitized.
I get your point, but it's really a stretch. There's been no reported cases of covid at our school and the symptoms matched common cold. Sure I guess there's a chance it could have been some mild case of covid the same as it could have been flu or some other illness.
Prior to the pandemic she used to be in a tiny school with 4-6 kids and 2 teachers and she was sick seemingly every other week. The difference seems to be the combination of teachers sanitizing everything, keeping kids in smaller groups, temperature checks, and parents not sending sick kids to school.
This is one of the problems with the newly-developed vaccines. It's not clear if they confer sterilizing immunity, so it's not clear if a smaller percentage of people getting the vaccine will stop the disease spreading. Therefore, it may be necessary to get most people vaccinated if we don't want the disease around at all.
I think the poster above you was talking about the chances of death from the virus, not simply the chance of infection.
I think it's pretty well established at this point that the case fatality index for children is vastly lower than for older adults, about 0.1% for people under age 29. [1]
And that's counting people who have bothered to get tested. If younger people are getting asymptomatic or minor symptom covid that looks like a cold, then the "true" ifr will be even lower
Infection fatality rates are based on antibody seroprevalence studies and thus accounts for asymptomatic cases. What you're thinking of is the case fatality rate, not the infection fatality rate.
Seroprevalence studies have been conducted all over the world. For example in Delhi India approximately 50-60% of the population now have antibodies for SARS-CoV-2. There are statistical techniques for adjusting the raw results based on population demographics.
Note that seroprevalence studies will underestimate the number of infections because some recovered patients don't produce detectible levels of antibodies.
No one will pay the political price of causing infections among children by reopening rapidly. And I'd like to believe that as a society, we are cautious about letting children be infected with a novel disease whose long-term effects are unknown.
Inflicting on all children the certain damage of social isolation, screen learning, and further economic precarity, to avoid theoretical and undemonstrated long-term effects (of a perhaps serious but not crippling nature) to a small percentage of them, does not strike me as societal wisdom in any way.
Also, do you know what else has unknown long-term effects in children?
I'm not arguing that children should be kept out of in-person school. In fact, I'm against it, and was against it even when the pandemic was raging last year. I agree with you that children have been silent victims of schoolteachers' refusal to do in-person school. I do, however, strongly support reasonable precautions including masking and physical distancing, which can be achieved with children (not very young children, but certainly 2nd grade and up) with continual reinforcement until it becomes a habit.
> I agree with you that children have been silent victims of schoolteachers' refusal to do in-person school
What should a schoolteacher do then, die? I'm not going to ask them to do that.
They should be put in one of the top priority categories for vaccination, and THEN we can expect them to go in classrooms (but we shouldn't be doing that anyway unless all kids are also vaccinated - otherwise they will keep the virus in circulation. They tend to have extremely mild or completely asymptomatic cases, but they DO catch it and spread it further)
Feudal traditions aside, no one has the right to draw an income from a position where they are not doing the job. So, if teachers don't want to teach, then they can find another occupation which they are comfortable doing.
I’m not sure your reading of the political climate is accurate. A lot of places have already reopened schools, and I’ve heard a lot of politicians explicitly say that they’re willing to pay the price because it’s not a big deal if kids get it. Maybe they’re wrong, but if you expect that there’ll be public support behind keeping things closed when the death and hospitalization rates start plummeting, I think you’d better readjust.
The Academy of Pediatrics says this. It's not just some politicans who don't know anything about epidemology and likely have never even taken a college-level biology course.
I'm not saying that places will be shut down completely. I was talking specifically about masking and physical distancing mandates and other such restrictions. I don't think big business and the public will tolerate losing another season of attending (in-person) Football, Baseball, Ice Hockey, <insert favorite sport here> games.
> I don't think big business and the public will tolerate losing another season
The whole "COVID fatigue" thing is one of the craziest things I keep hearing with regard to this pandemic. The virus doesn't care if you're bored of the disease and "won't tolerate" staying home from more football games. It's not like it's just going to go away because we're tired of it! I sincerely hope governments aren't going to just open things up because 2021 is a different year and everyone's just really bummed of it all. Surely we have better sense than that.
Avoiding getting Covid is not the only thing that matters in life. As the cost (in months of normal life lost) of the lockdown increases, it may be perfectly rational for people to think it’s no longer worth the decreased risk of catching the virus. Seen in this light, “Covid fatigue” makes perfect sense.
Said another way: imagine an alternate reality where none of the vaccines worked, and we kept getting winter flare-ups of Covid year after year - would you think we should continue the restrictions _forever_ ? If not, why not?
Assuming also that immunization did not emerge some other way also (like from getting the disease once) then yes I’d expect we would permanently change our way of life. What’s the alternative? Just accept the casualties year after year? For what? So we can eat at Olive Garden and go to football games?
How can you reduce all of human social and cultural life to “Olive Garden and football” ?
And yes, of course it’d be worth a slightly lower life expectancy in order to not live under permanent lockdown. If you don’t agree with that, we probably have such a fundamentally different worldview that we will never see eye-to-eye.
Since we're doing scenarios, what do we do when a hypothetical COVID-21 comes along which is 20x deadlier and kills uniformly across age ranges? Do we simply ignore it because we're tired of stay-at-home and we all gotta live our (now potentially shorter) lives?
Yes, if there were a virus that killed 10% of people of all ages and was as contagious as Covid-19, it would be a civilization-level threat and it would be worth extreme measures to attempt to stop its spread (I'm not optimistic that it _could_ be stopped, but it'd at least be worth trying). What's your point?
It's that fundamentally, our opinions are similar: There exists some point beyond which the threat is great enough to change our lifestyle permanently. We simply disagree about exactly where that point is.
By Springtime (in 45-60 days) we'll be at the one year mark, fatigued by masks, rules, shutdowns, and authoritarians, in general. The news will be tedious about how many are being vaccinated (it will be a lot) -- and, the weather will turn warmer.
Then, many/most will say _fuck it_, I'm taking my life back. I'm visualizing that day, and will welcome it.
I said "fuck it, I'm taking my life back" months ago. And then I realized how little that is possible.
How are you going to protest your way into a concert that isn't performing?
How are you going to demand your way into a university that isn't teaching?
How are you going to riot your way into a Disneyland that isn't running?
How are you going to force your way into a sports stadium that isn't playing?
How are you going to disobey your way onto a cruise ship that isn't sailing?
We are much more at the whim of our authoritarian overlords destroying everything joyful in life than we ever realized. We are no longer ever allowed to make personal risk management decisions.
> We are no longer ever allowed to make personal risk management decisions.
Your freedom borders with mine - you should be allowed to do EVERYTHING which doesn't affect others without their consent.
Ignoring COVID-19 precautionary measures isn't one of those things, and I am happy the joy-destroying authoritarian overlords took that choice from you.
That's just silly. By the same logic you could claim than no one should be allowed to drive cars, because an inattentive driver might kill you. If you're afraid then you're welcome to shelter in place alone for the rest of your life.
> you should be allowed to do EVERYTHING which doesn't affect others without their consent
People don't exist in vacuums. Nearly every decision you make is going to affect society somehow. If you decide to eat fast food for every meal and become obese, that isn't happening in a vacuum. Sooner or later you will start putting strain on the healthcare system and if enough people do the same, the "joy-destroying overlords" are going to start taxing sugar and fat (or other agency-limiting measures) to save you from yourself. Is that the world you want to live in - where the government has to increasingly limit everyone's agency in order to save more lives?
People can't do these things even WITH everyone's consent.
What if I and 500 of my friends want to have a comics convention? With everyone fully aware and accepting of any risks?
Nope, absolutely not allowed anywhere in the entire damn world.
It's right there in the US Constitution. "No law abridging the freedom of the people to peaceably assemble." It does not say "except in case of arbitrarily-declared forever-lasting so-called emergency." If you want it to say that, amend it. If such an amendment wouldn't pass, that's because it damn well shouldn't.
This is freedom-destroying authoritarianism, and the frightened sheep like you eat it up. This is where democracy breaks, if 51% of people want to lock down the other 49% forever, the other 49% are fucked forever.
If you fear contagion and think you need to stay away from me, that is on YOU to restrict YOUR activities. You do not get to restrict mine.
A higher number of people die of the flu and common cold every normal year because we don’t do lockdowns. Are you okay with that? Why or why not?
If not, then you must admit that, _of course_, increasing longevity to the absolute maximum possible extent should not be the only goal of public policy. And then it becomes clear that we’re talking about degrees. How many deaths are worth how much misery, suffering, and lost time among healthy people? Reasonable people can answer that question in different ways, but clearly the answer isn’t “zero”.
People should choose their own risk management decisions, not have a government forcibly do it for them. If you're concerned, you can choose to restrict yourself, but you have no business restricting me and any number of people that mutually wish to interact with me.
> We are no longer ever allowed to make personal risk management decisions.
Living life like there's no pandemic is not just personal risk, it's risk to other people and to society as a whole. If you don't understand that a year in, you're either not capable of understanding or you just don't care.
In a society many things we do expose others to some level of risk, even absent a pandemic. That risk obviously can't be zero. So please quantify the level of risk we should be allowed to create for others.
Obesity and heart disease have been killing far more people in the US than covid and yet Mcdonalds and Coke advertisements are everywhere inbetween television entertainment.
Also note obesity/heart disease are among the greatest risk factors of poor health outcomes for covid.
Why is there little to no mention of eating healthy and exercising in the government's health guidelines to combat this threat?
There are countless other examples of bureaucrats caring more about money and power than public health - while putting on the appearance of caring for public health. See also: the war on drugs.
Overeating and poor exercise only hurts yourself. The difference is that you going to a concert, contracting corona and passing it around our household/workplace may kill somebody completely unrelated to the initial risk vector, how would you feel if your neighbour eating McDonald’s directly affected your health?
Even before coronavirus, going to a concert, contracting influenza and passing it around could have killed someone. Influenza kills thousands every year, asymptomatic transmission is common, and the vaccine is only partially effective. COVID-19 is significantly more deadly but that's just a difference in degree; the same fundamentals still applied. So by your logic apparently concerts shouldn't have ever been permitted at all.
Corona is substantially more deadly, and long term effects can be permanent, it’s also in addition to the flu. By your logic we should just let corona run it’s course? You’re willing to let others die just so you can see a concert?
We can all ask ourself : How many time I would accept to be confined now to live one more day/week/month/year at the end of my life. Now we can use this ratio and apply it to our current choice to calibrate how much we stay confined.
Isn't it better to live life fully when we are young and healthy, than to hide inside our homes in hopes for an extremely small chance that we might have a little extra time when we are old and decrepit?
Seems like this ratio would vary greatly among such demographics.
>Overeating and poor exercise only hurts yourself.
Obese people are twice as likely to be hospitalized for covid.
When hospital beds are being overrun, someone elses life long decisions to disregard their own health does indeed affect other peoples health negatively.
Are you into apocalypses? There's the British quick-spreading strain, and there are the Brazilian and South African variants that the vaccine does not offer good protection against. I predict that COVID will be like Picardy Fever, not like the Spanish Flu - there will be outbreaks every few years here and there.
The apocalypse scenario is unlikely with the population having some resistance to the virus after vaccination even if new variants possibly render the vaccine less effective. We obviously do not have enough data yet to understand the vaccine's efficacy against these new strains but a lot of scientists are saying it will be "good enough" while we work on vaccines to handle the variants.
If this thing can basically be treated no differently than the common cold once vaccinated by most people and in the outliers something a little worse there will be no popular support to continue draconian lock down measures.
The goal is to stop the bleeding. The patient is on the floor right now and haemorrhaging liters blood. We want to stabilize the patient and let them get on with their life as quickly as possible. We cannot let perfect be the enemy of "Good Enough" here.
Agreed. Hospital overflows is the main issue - and we know that things are far worse in winter than in summer. Come May things will be heading back to normal, and hospital collapse won’t be the concern it was this year come next October due to widespread vaccination.
At least in the west, global logistics of vaccination seem to have collapsed. We need to, as a species, get on top of vaccine rollout for next time. It’s delayed at the moment because we didn’t make enough vials over summer FFS.
Global eradication of diseases is very hard, because there are lots of areas that don’t have much money or government capacity to dedicate to disease control. Developed countries have brought quite a few diseases to near-extinction within their borders; tuberculosis is the obvious comparison, given the similarity in symptoms, transmissibility, and vaccine efficacy.
You'd be surprised with respect to tuberculosis. We use a vaccine developed 100 years ago, a vaccine which actually doesn't really work in adults (and immunity from the vaccine gets lost by adulthood), and antibiotic resistant strains are only becoming more prevalent.
Doesn’t seem like that condition leads to termination. As things return to normal, fewer surveillance tests will be conducted by definition, so the test positivity rate will rise.
In BC we've learned that we need to distinguish between the positivity rate for "testing due to symptoms or known exposure" and "testing for screening" (e.g. the film industry tests all their crew daily). The former positivity rate is much higher, but the latter may be more useful as a long-term trendline to follow.
Test positivity is a weird metric because of things like this. It's interesting week-over-week, but loses meaning over the long term as testing protocols, other behavior changes, and changes to the disease. This makes it a lousy metric for policy making.
There was a county in Louisiana that went back into a shutdown Thanksgiving week, when nothing at all had changed, except that a local university was on break and had stopped flooding the daily statistics with thousands of negative tests.
Not to mention the perverse incentive: if you feel sick, you want to avoid getting tested and counted as a positive if you don't want your locality or employer to shut down. There is a theory that this accounts for much of Japan's perceived success - antibody studies show just as much prevalence as everywhere else, what happened was that all the mild cases never got tested.
There are also non-perverse incentives. If I feel sick and live alone, a test test result doesn't give me much actionable information, takes time, and puts the people giving the tests at slightly more risk.
I don’t think it matters if 100% is vaccinated. What matters is new cases and deaths. As long as those are steady or going up we’re going to be masking and social distancing until the end of time. Once it goes down and stays down, that’s when gradual rule relaxation happens, and mass vaccination is the hoped-for silver bullet for it
According to this yahoo article about 65 - 70% of the population needs to be vaccinated until we can get back to normal. That said there still may be mutations or other complicating factors that could throw a wrench in things.
Research suggests that after infection with some coronaviruses, reinfection with the same virus — though usually mild and only happening in a fraction of people — is possible after a period of months or years. Further research is needed to determine the protective effect of antibodies to the virus in those who have been infected.
Even if infection with the COVID-19 virus creates long-lasting immunity, a large number of people would have to become infected to reach the herd immunity threshold. Experts estimate that in the U.S., 70% of the population — more than 200 million people — would have to recover from COVID-19 to halt the epidemic. If many people become sick with COVID-19 at once, the health care system could quickly become overwhelmed. This amount of infection could also lead to serious complications and millions of deaths, especially among older people and those who have chronic conditions. [1]
Which would result in ~1.3M dead Americans.
So no. The concept of defeating COVID by relying on a "natural herd immunity" is a bad idea on all fronts.
What should I tell my elderly relatives who are so creeped out by this fascist, disgraceful fiasco, that they will refuse a vaccine even though it has a decent chance of doing some good?
Thank you. My grandma tested positive on a Monday around a month ago and went into hospice the following Thursday night, when her oxygen dropped. She passed away the following Saturday morning.
My girlfriend's grandma also passed from COVID a few weeks ago. When it rains it pours, eh?
The whole thing is just horrible to deal with. Not having a chance to say goodbye or go through the grieving process together.
It's just so hard to comprehend how 419k+ other families in the US have experienced similar loss.
Same here. My grandfather died early in the pandemic (May). He tested positive for a period of three weeks and then tested negative a few times. He started feeling better and we were hopeful, but the damage was too great and his heart failed a few weeks later.
I really just can't put my feelings into words.
He was in a physical rehab facility after surgery. When the pandemic hit, visitation was forbidden. Turns out most of the staff were scared and basically abandoned the patients. The specific facility specialized in elderly patients who had severe mobility issues.
He told us on the phone once at the beginning that he was scared because all he heard at night were people screaming for help as they stopped being able breathe as COVID was destroying their lungs. He figured it wasn't long before he caught it. However, no one would sign off on discharging him, and by the time we got the bare minimum to care for him at home and the legal crap sorted out, he caught it.
He lived practically opposite the country to me (I'm in LA, he was in Boston), so I didn't see him very often. He also wasn't the kindest person to me growing up, so I didn't really talk to him all that often either.
With that, it just doesn't feel real that he's gone. There was no funeral, no memorial service, as everything is tabled until after the pandemic. I don't think it'll really set in until I visit my grandmother and he's not there.
And you see the assholes who want to say taking precautions should be a personal choice or are an invasion of their personal freedoms. I wish every single one of them could experience the fear my grandfather did. Stuck in a bed, unable to walk, waiting for a plague to take them as their fellow patients succumb one by one. It's just disgusting.
My grandmother, wearing a full hazmat suit with an oxygen tank, was able to be there with him when he passed.
I am at the same level of loss-shock as you, I suspect. My mom lives and my grandma lived on the Iron Range in Minnesota, so a very rural area, which seemed to help keep infections at bay for a while.
It's been incredibly hard for my mom, because my grandma was her best friend and her rock. The day she passed, I remember my mom saying "I never got a last hug", which was heart breaking. My mom has MS, so there was no possibility of her visiting her through that whole process.
It's been really hard. I want to see my mom and give her a hug. But I also don't trust the time in between getting the results of a negative test to feel confidant about visiting her.
Hopefully we'll all find some closure once we have a chance to grieve together, properly. There are many memorial/celebration services that have been postponed. I hope we can reach the day where we can hold them safely together.
Thank you for sharing, really, but understand that I could also slip into blind hatred over what I see as the suffering you and your culture have caused (not least being caregivers so scared by the hyped-up risk to younger and healthier people that they abandoned patients?!) but that would not be useful. As the minority opinion I’m also more likely to get flagged or banned, and I do use that handicap as a crutch sometimes (thanks @dang).
Perhaps the best option would be for us to get drunk and rage about this for a few hours or days. I bet I could rant for a lot longer than you, and I bet I understand your position better than you understand mine. Perks of being in the counterculture, I guess.
I feel like your point is probably important somehow. Could you make it with more sensitivity and less indignant contrarianism? Remember that you're replying to someone who has just lost a loved one!
Someone who in their grief also wishes me suffering and an agonizing death, perhaps as revenge:
> I wish every single one of them could experience the fear my grandfather did. Stuck in a bed, unable to walk, waiting for a plague to take them as their fellow patients succumb one by one.
Sensitivity is a nice-to-have, but the goal right now is averting outright war. If none of these bubbles can be cracked open, and everyone just keeps lurching toward violence, where it ends will make today’s tragedy look like mild inconvenience.
Please note I specifically said I wish they could experience the fear. It is not a wish for anyone to experience death, let alone a painful one.
People rarely have to confront the extent of the results of their actions and as a result don't really think on those terms. Personal experience is an effective, often painful teacher.
I can't claim to know your entire perspective, but from the outside, refusing to accept a temporary, minor inconvenience to one's life so we can reduce how many people have to die an agonizing death seems ... selfish, at best.
I myself am a person who suffers from depression issues that have only been magnified by isolation. And yet here I am, following the guidelines as best I can. I'm not at much of a risk of dying from COVID, but if I got it and infected someone who ended up dying from it - I'd never forgive myself.
Thanks for the reply. And er, good that you don’t actually want to go as far as killing me - there’s some wild shit out there right now. I would still be in favor of arguing about all the details over drinks, but for now I’ll just offer the roughest outline of the other perspective, which is:
Refusing to accept a temporarily increased risk of disease, and instead dramatically increasing the chance that your fellow humans will be crushed under the boot of fascism is... also selfish at best.
Ah, you're one of the ones who actually is rational about things.
Put it this way: your liberty to spread your germs ends just where my nose begins. Else we're just permitting tyranny by another route.
Currently there's a very infectious and deadly germ on the loose, so -under the above rule- everyone's freedom becomes more constrained than we'd ideally like.
It's certainly evil; but it's not the human evil of fascism causing it, but rather the natural world evil of a pandemic.
You exhale viruses. You exhale CO2. The campaign to remake society in response to these threats is, in its purest essence, a campaign to redefine the free human as a toxic animal. If successful, it will then be used to justify slavery and murder.
And to borrow a page from the global warming folks, we’re not going to wait and see whether that hunch is right, because by then it will be too late. It’s time to end this.
The USA actually dealt with a similar situation just over 100 years ago in 1918, and people did similar things, and the USA came through just fine as a nation (albeit 600000 citizens lighter :-( ) .
If you don’t already understand that argument as a perfectly obvious concern, we will probably not agree. It is obvious to hundreds of millions, probably billions, of people all over the world.
I recommend you look for conversations outside your usual bubble, and when you find someone to ask questions of, don’t pair the questions with insults.
I don't think I can excuse abandoning patients, but not all caregivers are young and healthy; so some of them would have reason to fear for their safety, or the safety of those they live with, or not want to spread disease among their patients.
Lots of stuff went wrong, and it's tragic that
Teknoman117's grandfather couldn't get discharged quickly. It would have been better to be at home without appropriate mobility care than to be in a facility without appropriate mobility care and an active outbreak.
My grandma too. A week from first positive test to dying. It must have been very scary for her. No funeral. I found the part that continually makes me melancholy is all of these people alone in the hospital, separated from family, and feeling themselves get worse and worse.
Death is quite natural, but the fact that a single pathogen, which other "western" nations managed to get under control has become the second leading cause of death in the United States is a horrific thing.
Heart disease is a systemic issue of our lifestyle and diet, and we don't know how to prevent cancer. A pathogen is fairly simple by comparison - if you don't catch it you can't die from it. Prevent the spread and people won't die from it.
Except other western countries haven't "gotten it under control"... they are all having second waves and resurgences with or without large lockdowns and with or without draconian processes.
> fairly simple
Until you start looking at how many lives are saved vs the second and third tier effects. Higher suicide rates from losing jobs and stress? People in third world countries dying from a cratered world economy? etc.
COVID needs to be handled and those more affected by it need protected. More hospital prep and masks around grandma... but the "fascist" and unproven shutdowns which by any measurements not only don't work but - as mentioned - causes more damage than it prevents?
Lockdowns, social distancing and masking – done consistently – do work. Even the half-measures lockdowns the US has gone through has stopped the entire medical system from collapsing, and at times it has been very close. In NYC in the first wave, it did.
But that isn't what has happened in the US, largely for political reasons.
There are no good options, only less worse ones, and aggressive lockdowns have got Australia, for example, back to work. The cumulative cost of the US's failure to grasp the nettle and just shut everything down for two months properly back last March is enormous.
and yet states that didn't - and aren't - locking down - like Florida - are doing fine. Or better than states that have extensive lockdowns like New York, New Jersey and California...
> Political reasons ... aggressive lockdowns in Australia
Locking down a small country like Australia is much different than locking down a country like the US. Australia is only 20% smaller than the US yet has 10% of the population. The layout is different. Temperature. Density. etc.
Locking down Australia would be like locking down one of our less densely populated states - not only does the President not have the ability to do it - he's a President not a King... but locking down the country make zero sense for a virus with a 99%+ survival rate.
again... we can take precautions to protect our hospitals and to "flatten the curve" (which we are loooooong past) and to protect the vulnerable (old, existing conditions, etc)... but locking down America? Coast to coast? No chance this side of turning the President into a Dictator - which was never on the table for Trump and definitely not for Biden.
> Locking down Australia would be like locking down one of our less densely populated states
This is very wrong. Australia is very, very dense, where people live: it just has a lot of absolutely uninhabited land. Functionally Australia is almost entirely urban.
Yea, Florida is not "doing fine" by any stretch of the imagination. It's just that they don't want to report numbers that show them not doing fine, as the entire state is funded by tourism.
They seem to be doing a pretty good job with vaccination though, so there's that!
Australia has had recorded zero locally acquired cases for more than 7 days now. At one point, Melbourne recorded 700 cases in a day, after several months of hard lockdown, it's down to 1 case in 30 days.
Yep, and Melbourne had it's "second wave" in the middle of winter. Locked down and got it under control. We've had the opportunity for things to go pear shaped, but due to decisive action, an educated and thinking public and fairly strict enforcement we've got no community transmission. The only issue we have is that our methods of isolating people returning to the country are proving to be somewhat inadequate with people like cleaners picking up the virus from the isolation facilities (Hotels). These issues are being improved and it looks like we are going to continue to be virus free.
And depression can be a slow killer, I’m more interested in the 2020 numbers for strokes and heart attacks. People have been hesitating in emergencies for almost an entire year (and counting).
Living on the border of two such western countries, I'd like to point out that they are definitely taking measures (currently lockdowns) to keep things under control, the lockdowns have a very measurable effect on R, and the death rate in both countries is something like 1-2 orders of magnitude less than the USA.
Basically you're trying to control R. As long as you keep R under 1, you can increase and reduce measures to keep the disease under control. If R goes too far over 1, you bleeped up, and you need to resort to a lockdown to get it back under control.
The theory a lot of (european) western countries are working on is that they want to allow as much freedom as possible, but keep the worst of the disease out.
I'm not entirely convinced this is actually the strategy that optimizes freedom though. It might be better to use the method some asian countries used: close the borders, do maximum effort lockdowns anytime the virus shows up at all; and you might have less days total in lockdown or restrictions, and more days where you are free to go out and eat indoors etc.
The one huge tragic problem with that plan is that when we surrender our freedoms “temporarily” to the government, they never give them back! Or at least we do not trust they will give them back, based on vast experience (see: Patriot Act), so this plan cannot work.
The naïveté on display here is staggering. "You can vote your way into fascism, but you have to shoot your way out."
In other comments people pointed out that New Zealand followed this more stringent strategy.
Right now, they're all outside enjoying summer with almost normal freedoms, while we're still stuck indoors. I must admit I'm jealous!
I don't think the Kiwis are currently preparing to shoot their way out of anything right at the moment. Probably because they're pretty much free to do whatever they want.
I will grant that New Zealand had an easier time of it as an island nation with a low population density, but it does give you pause for thought. Maybe we all could do better next time when the next pandemic rolls around.
Oh for sure. Grieving over death in 2020 is just all around a bad experience.
But I think it's fair to say that the excess deaths [1] in 2020 have certainly amplified the reality of death, especially within the context of a shared experience. My grandma was otherwise healthy and I had had a lot of conversations with her about how much we looked forward to seeing each other once the pandemic was "over".
Right, that's my point is that death sucks and it happens a lot. Obviously we would love to prevent all the death we can but just living is not always a good trade off. My grandma for example hasn't been allowed visitors for basically a year and says she would rather be dead.
I’m not sure how much of it is fear of the MRNA vaccine itself, and how much is an objection to the creepy fascist context. Probably a lot of both, and maybe yes a bit too much of the former.
But in any case their reply is, “We would rather take the risk.”
If they get sick and die like your grandma (condolences), they will have done so at least partially by choice, a choice which they have damn well earned by their mid-nineties. I would not prefer that to them avoiding the disease entirely (they would be especially mad at being shut away in a closed ward to die alone), but it sure as hell would still be better than seeing them enslaved by technocrats.
You could encourage them to keep in mind that by refusing to get vaccinated, they're likely going to be living the rest of their life under threat of contracting COVID.
It seems that those who are vaccinated can still spread it, and I don't believe we're going to be in a place where COVID is eliminated altogether anytime soon. There will continue to be outbreaks, and it's possible that those who are vaccinated will pick it up and pass it around, and the further mutations of it seem to be increasing its rate of spread.
> You could encourage them to keep in mind that by refusing to get vaccinated, they're likely going to be living the rest of their life under threat of contracting COVID.
I think you might be blind to how a person who values freedom more than safety, and who sees more danger to free civilization than to public health in this affair, would receive this threat. It would be an utterly awful thing to say.
I agree that my understanding of that mindset is limited to the rationality I can make of it, but I wouldn't consider that a threat. It's the reality that we exist within, as this virus only really "cares" about replicating itself.
I personally don't comprehend how someone can extrapolate receiving a vaccination to a loss of freedom, but I'm fortunate that I don't really have to.
Best of luck and safety to you and your family. I look forward to the day that we get to begin returning to some semblance of normalcy. Hopefully it's sooner rather than later.
Thanks, same to you. Don’t count on any “return to normalcy” though, at this point the only way out is through, and the other side is gonna look a lot different.
Let’s grant that one thinks that the various COVID restrictions are a danger to free civilization. How exactly does this translate to getting a vaccine being a danger to free civilization?
The funny thing is that a lot of the measures are based on either bad science or not science at all. Still, the masses will tell you to fall in line and accept the meaaures because "science says so". If you ask them to explain the scientific method on the spot 99% won't be able to do so. No wonder why they're so easily fooled. The "experts" are the new priests and science is the new religion. And don't you dare question it.
Have you considered relocating them to New Zealand? No COVID, no masks, no need for a vaccine. I’m not sure about government overreach in other parts of life though.
It's not just NZ. Australian states have carried out similar decisive actions.
An example. We had one person in Brisbane (capital of Queensland) who was infected with the UK variant whilst working in one of the isolation hotels (used to isolate people returning to Australia for 14 days).
The infected person reported that they had travelled extensively through the greater Brisbane area during the previous days. Given the unknown factors around the increased ability to transmit of the UK variant, the Queensland government called a 3 day lockdown on Brisbane. No travel unless absolutely necessary (food, medical care, critical job) and if you were outside your house for any reason masks were required.
The three days were to allow the health department to trace all the contacts of the infected person and get them tested. General public were also told to get tested if they had any symptoms and testing facilities were reactivated across the area.
Three days later, no new infections and the restrictions, only retaining the mask mandate in confined areas for another three weeks. We are now about three weeks later and no new community cases.
So was the three day lockdown excessive. I don't believe so. Would the outcome have been any different if we didn't have the three day lockdown? As it turns out, probably not, but it has to be noted that the purpose of the lockdown was to force a stop in possible transmission and give the health department a chance to find out how many people had been infected. Turns out that the infection rate was very low (some immediate family).
If we'd found from the tracing that there was active community transmission there would have been an extension to the lockdown until the rate reduced.
But here we are, essentially living lives unrestricted our freedoms intact until the next time this thing escapes into the community. Then I trust that the government will take prompt action and the public will groan but comply and we will be inconvenienced for a short period before we again return to normal.
Australia has learned a lot about what works and are acting on it. I don't know what lessons can be transferred to the tragic situation in the US apart from showing what would have been possible if your government had taken this seriously from the start.
I feel very sad for your country and wonder how the greatest democracy on the planet has allowed individual freedom (if you want to call it that) to be considered so important that it has been allowed to compromise the freedom of all.
> I’m not sure how much of it is fear of the MRNA vaccine itself, and how much is an objection to the creepy fascist context. Probably a lot of both, and maybe yes a bit too much of the former.
I don't think the two concerns are all that neatly separable. I find it impossible not to notice the relentless campaign to put forth _vaccinating everyone with an experimental jab_ as the only legitimate escape from indefinite lockdowns and distancing. Evidence piles up in favor of easy & cheap measures like vitamin D supplementation or ivermectin treatment having the potential to significantly reduce the threat of Covid and it just gets drowned out by media noise.
I view mRNA vaccines in much the same way as nuclear power: they could be an important technology to address our problems, if we could trust our institutions to adequately guard against their potentially enormous hazards or misuse. But we can't. And while I haven't decided yet whether I'm going to get the vaccine, one thing that will make me much more likely to fall into the "refuse" camp is if they decide to impose some kind of restrictions on basic freedoms and make travel or attending concerts contingent on getting a vaccine.
Even with all these concerns, if I was in my 90s, I think I would still find the danger from Covid so severe as to tilt the risk/reward balance in favor of getting the shot. But I don't find your relatives' approach absurd by any stretch.
> I don't think the two concerns are all that neatly separable. I find it impossible not to notice the relentless campaign to put forth _vaccinating everyone with an experimental jab_ as the only legitimate escape from indefinite lockdowns and distancing.
Who said that?
There are quite a few ways out: we can reach a state of herd immunity (as a practical matter, this would mean that going back to normal would result in a low enough rate of serious infections as to not be a big deal), we could find an effective, practical treatment or prophylactic, or we could vaccinate everyone. Or a combination.
Many things are wrong with the process, but, right now, all credible models suggest that we are nowhere near herd immunity. We have two vaccines that, in proper RCTs, appear very effect. We have a third vaccine that had an incompetently run RCT and appeared somewhat effective.
As for other treatments, we have some things that help a little. There’s ivermectin, which (if you read Derek Lowe’s blog, for example), seems dubious. It’s cheap and safe, but the dosage that works in vitro is impractical in vivo. The studies saying it’s effective are, in my opinion, dubious. Vitamin D (injected) looked good in a tiny study. Fluvoxamine looked good in a well run but very small study. HCQ does not appear effective. Convalescent plasma looks so-so. The mABs look less effective than hoped, and they don’t really scale well enough to use for everyone who gets exposed. Remdesivir seems to be barely effective.
We should absolutely run serious, expedited trials of everything credible. The fact that we haven’t set up a national clinical trial system for this is an embarrassment.
But please check your assumptions. Under the previous administration, the federal government did not impose significant restrictions on your freedoms (even your freedom to go around in indoor public spaces without a mask). The government did not do much of anything useful. To the contrary, the government gave premature EUAs to untested treatments that actively interfered with the private sector’s ability to run trials. The current restrictions have been largely imposed by the states, democrat and republican, whose governments have been some combination of ill-equipped to do anything else and insufficiently creative to come up with anything better. There is no “they” setting up a campaign to convince people that the new vaccines are the only way out. Heck, there isn’t even a “they” doing a good job of jabbing people at all — note the bizarre contrast between the number of doses shipped, the number administered, and the medical providers who have run out of doses.
If you want to look at a country with an organized vaccine campaign, try Israel. If you want to look at countries that are managing COVID effectively with minimal invasion of peoples’ freedom, look at Taiwan, New Zealand, and China. (China has taken extremely harsh measures, and their administration is not dumb. Taiwan’s measures are not particularly harsh. All of these countries have serious travel restrictions, which the US states cannot implement on their own.)
W.r.t. vitamin D I was referring to supplementation to prevent deficiency in the first place, not to administering shots as treatment to desperately try and get the levels back up once an infection reaches an advanced state.
I find any "the required dose for in vitro neutralization is too high" reasoning to be dubious for the simple reason that we are not trying to battle the virus in vitro. A good meta-analysis on ivermectin: https://www.researchsquare.com/article/rs-148845/v1 There are also some accounts of possible successful use as prophylactic in Chiapas and India but I'm not familiar with any studies on that subject.
I don't really feel any cognitive dissonance in observing that the same TPTB (if you prefer that term to "they") which clearly strongly desires that everyone gets a jab is not necessarily all that competent at running the administration and logistics side, particularly not on the enormously compressed timescales which have characterized Operation Warp Speed.
Japan used to be included in the usual lists of "here's how it's done" countries until they had some relatively significant community spread this winter. New Zealand has been in their summer but just reported their first case of community spread in months as their autumn gets underway -- being an easily isolated island I imagine they might have more success keeping things under control, but if Covid goes endemic I don't expect lockdowns to halt it in its tracks there any better than they have in the US or Europe. I don't buy China's numbers given that they have laughably reported a single Covid-19 death for a country of 1.4B people in the last 8 months, and find including them on a list characterized by "minimal invasion of peoples' freedom" bizarre.
A good place to start to reduce the number of infections would be to work out a proper test. With PCR tests you can modify the number of cycles to fit your goals, from "serious pandemic" to "we are almost case free" within days. Also it seems like these tests test positive for people who have been infected months ago, so it's more than likely to pile up the numbers of cases even though most of those aren't really active anymore.
> And while I haven't decided yet whether I'm going to get the vaccine, one thing that will make me much more likely to fall into the "refuse" camp is if they decide to impose some kind of restrictions on basic freedoms and make travel or attending concerts contingent on getting a vaccine.
Ding ding ding, I’m already refusing in solidarity with anyone else who wants to refuse for whatever crackpot reason they like. The system pushing the vaccine is far too corrupt, and the bullying is already far too aggressive, to justify any other position. But it is still a tough decision, because the expected risk of war and fascism is pretty fucking hard to calculate.
By the way in a vacuum I like both MRNA vaccines and nuclear fission, despite the risks.
Perhaps if you encourage them to think of it as something other than a creepy, fascist, disgraceful fiasco, they might be more inclined to think rationally about it?
Not buying that for a second. This same industry ran PR to squash efforts at developing competing vaccines in human challenge trials[0]. I try to remind myself that most individual players don’t act with malice, but the system as a whole runs purely on profit-taking and corruption, and it has managed to do horrific damage.
Lots and lots and lots (hundreds of thousands) of people in Russia have been officially infected and diagnosed twice. Many Russian docs who worked with Covid patients have already been sick three times.
And yes, most of the time they say it's 3-5 months for asymptomatic cases and 9 months and more for severe symptomatic.
It appears that Russia has a different distribution of coronavirus strains than the rest of Europe [0], but the strains in Russia are certainly found elsewhere. If hundreds of thousands of Russians were re-infected this would be observed elsewhere and documented.
The closest thing I can find to reporting on this matter is here [1]. The Siberian Times does not appear to be a reputable news source [2], and its claims do not match the magnitude of those above. It reports that Russia’s chief sanitary doctor Anna Popova said, "in Russia there was not a single confirmed case of coronavirus reinfection." Furthermore, the doctor on the other side of this disagreement has "heard about other cases [of re-infection] elsewhere in Russia from colleagues" (and claims to have been re-infected).
This is not "lots and lots (hundreds of thousands)"...
There is evidence of re-infections in the scientific literature, but they are exceedingly rare (tens of people worldwide). Long-term immunity will have to be measured, especially in light of new variants, but current evidence points in that direction.
Do those kind of calculations assume that the people who are vaccinated are spread fairly uniformly throughout the population, or do they take into account that people who will not take the vaccine will have a tendency to clump so that we are likely to have some cities or counties with high vaccination rates and other cities or counties with low vaccination rates?
That number has been thrown around for here immunity. But I don't think it answers the GP's question because
* Herd immunity numbers assume no ongoing vaccination -- they more or less say, "If life went back to normal, would the virus slow down or speed up?"
* Age-related mortality and age-related vaccination rates are important. If we vaccinate all of the people who are at serious risk, the danger is mostly gone. There have obviously been deaths in populations not at serious risk, but not in proportion to the economic costs of locking down the economy.
And as an aside, vaccine immunity is estimated to be about as good as post-infection immunity. And most estimates of the actual infection rate put them several times (some estimate 8-10x, but that's looking unlikely IMO) the measured case rate.
Imho you’re underestimating the impact of the disease in general. Disease is much more than who lives or dies, there’s also people who “survive”. A number of asymptomatic covid patients have severe lung damage. Vaccinating “at risk” people who might die doesn’t account for all the people who might live permanently disabled lives as a result of a covid infection.
Dying from Covid is not “asymptomatic Covid”. So your evidence for this phenomenon consists of a local news article where they’ve quoted the opinion of one person, mis-represented a figure from a journal article, and showed x-rays with no citations or context.
There are three X-rays in this article, and the covid one is completely bogus. Kind of stains the credibility of the article and the company the produced it.
Considering the source for that is a single trauma surgeon on Twitter, I'm going to wait until there's something formally published on the matter. We have no information on the condition of the patient with "covid lung", or even a comparison between asymptomatic patients vs patients put on ventilators. Not saying you're wrong, but that article seems sensationalized and quite honestly lacking in relevant information.
That will depend heavily on what state you are in. Dining in is fully open in some states with only masks on entry/exit. Mask usage in some areas is vastly different than others.
Its likely that a some places will heavily ease restrictions as soon as next month.
The people getting vaccinated right now are those that are, by far, most at risk. Every single extra vacation right now has a high chance of saving a life, which is much less true for the vaccinations that are administered when reaching the numbers that you care about.
Also, I don’t know where you live, but I think in most places on earth you can legally have dinner with a small amount of friends, without some “influential” person giving you permission.
Not the case UK, and from what I can tell much of Europe is not allowing that at present either.
Here in the UK you may only meet other people for exercise purposes, outside. No visiting each other's homes. It's been this way in most parts of the country for months. Same in Ireland
In France there is a curfew from 8pm-6am and restaurants cannot open. There have been rules preventing meeting others at home, can't tell if they're active right now.
In Germany one person not of that household may visit another household, but only one. This is also true in Belgium.
Some areas of Spain are not allowing meeting in others homes at all.
Not here in Israel. We're in our third lockdown and they keep extending it (it was supposed to be two weeks...I can't keep track of how many times its been extended).
I was sitting in the park in a riverbank the other day, cops patrolled and asked people where they lived. Whoever you're with must live in the same household as you, and you may not be more than a km from home. I didn't see anyone get fined (although I believe they have the discretion to do so) but I saw some groups of friends be dispersed by the police.
The masks will stop as soon as people stop wearing the masks, I expect that may need to happen before politician’s “cover my ass” mandates are abandoned.
The vaccine grants 95% protection with those measures in place. We have no idea how effective it is without those measures. If we're all going to dance parties, the vaccine might not be adequate.
I think the question is the point at which we can send kids back to schools and reopen our businesses with precautions in place -- in other words, stem the pain and bleeding.
It makes sense to keep masks on and 6-foot distance until the virus is gone, though. Vaccine+masking/distancing should be enough to get rid of it. It's not clear vaccine alone will do that.
If not, we'll be on a dance for decades with new mutations, vaccines, and whatnot. We want this thing dead and gone for good.
I don't think we're on a path to get there, though. People are fed up. If we can't get this under control, I suspect the new normal will be outbreaks for the rest of our lives. Perhaps the vaccine will be 95% without distancing. Or perhaps not.
>Vaccine+masking/distancing should be enough to get rid of it. It's not clear vaccine alone will do that.
The public is treating the vaccine for like the vaccine for polio, which is that once you get it, you're good. If 80%+ of Americans get the vaccine and we still have to mask and social distance, you're going to see a lot of angry people.
>If 80%+ of Americans get the vaccine and we still have to mask and social distance, you're going to see a lot of angry people.
Then people need to do better. Getting angry at reality doesn't change it. If this is how things work out, throwing a fit only makes the situation even worse.
Carl Sagan once pointed out the perils of basing a society on all this science and technology, when only a few people (relatively speaking) actually understand it. I didn't truly understand this warning until this pandemic.
We've seen a lot of angry people. Prior to COVID19, I was quite frankly unaware of just how good Americans had become at denying reality.
When COVID19 hit China in January, it was clear it was coming to the US. At the time, I thought the US government was preparing. Nope. Complete denial.
When it hit in March, I thought schools would prepare. Nope. Complete denial. It's 2 weeks. 4 weeks. It'll be gone come the summer.
And so on....
... Anger against reality has led to over 400,000 deaths so far.
No one is quite sure but we're a LONG way from it.. and that's without addressing the fear/trauma that's been inflicted on otherwise healthy+exceptionally low risk people.
From a month ago:
Dr. Anthony Fauci now says as much as 90 percent of the population may need to get vaccinated or infected to achieve herd immunity against COVID-19 — admitting in a new interview that he has been intentionally raising the bar based, in part, on what he thinks the country is ready to hear.
“We really don’t know what the real number is,” the nation’s top infectious disease expert told the New York Times.
“I think the real range is somewhere between 70 to 90 percent. But, I’m not going to say 90 percent.”
He does have a track record of being dishonest about things. Part of the reason he drug his feet on masks was he was worried about shortages. It makes sense, but I really don't like the "I know what's best for you" paternalism.
Fauci was never dishonest. That was Trump trying to shift the blame to him. Watch the original clip: https://www.youtube.com/watch?v=PRa6t_e7dgI&feature=youtu.be He literally said that the reason he is advising against masks was because he was worried about shortages.
TheStreet asked him "why weren't we told to wear masks in the beginning?"
> Well, the reason for that is that we were concerned the public health community, and many people were saying this, were concerned that it was at a time when personal protective equipment, including the N95 masks and the surgical masks, were in very short supply. And we wanted to make sure that the people namely, the health care workers, who were brave enough to put themselves in a harm way, to take care of people who you know were infected with the coronavirus and the danger of them getting infected.
He didn't say "because we didn't know any better," he said (paraphrased) so the general public doesn't go out and buy them, causing a shortage. I find that dishonest.
Another example, when Trump (like him or not) pretended to be best pals with Kim Jon Un, he was being diplomatic. CNN accused him of being dishonest and called for him to announce publicly to his country that "actually I'm lying".
Was he 'lying'? Yes. Should he have told the truth to Kim Jon Un's face for the sake of 'honesty' and destroy all the diplomatic progress he had made at a time when KJU was flaunting his nukes? Maybe. Probably not.
Back to Fauci. Was he 'lying'? Yes. If he had told people 'masks work and will save your lives but health professional lives are more important' would that have had the same effect? Maybe. Probably not.
Also, since we love our fallacies in this place. Accusing someone of being dishonest for no good reason is effectively a variant of the outcome fallacy (judging the quality of an argument/action based on knowing the eventual outcome, rather than judging whether it was a reasonable course of action given what was known at the time). We simply do not know had Fauci been 'honest' whether the death toll would be halved or doubled right now. We can only speculate.
Your first link says not to unless you're sick, implying that they thought they were useful for people with the virus. The second link literally says that having supplies for healthcare workers was the main impetus for saying this.
This has stood up remarkably well, a year on we know that masks are mostly effective to prevent people spreading the virus and not to prevent contracting it and we know much more about how readily it spreads asymptomatically.
Fauci was pretty explicit about it in the linked interview:
> “When polls said only about half of all Americans would take a vaccine, I was saying herd immunity would take 70 to 75 percent,” Dr. Fauci said. “Then, when newer surveys said 60 percent or more would take it, I thought, ‘I can nudge this up a bit,’ so I went to 80, 85.”
I think it’s fair to characterize this as dishonesty, and to be less charitable about whether his past communications were in retrospect honest.
Every medical professional I know /am related to has indicated that getting covid only grants 90 days immunity. Across state lines, they all have said that herd immunity visa infection is impossible as it requires everyone to be infected within a three month span.
This is charitably a misconception, and very possibly an outright lie. Nothing indicates a 90 day cutoff to immunity. On the face of it, that should make anyone reading this sceptical.
I was very skeptical of it as well, and had the same reaction to the medical professionals saying this. Their off the cuff "oh, yeah, ninety days, makes sense" led to me believe them. Note as well I'm referring only to catching covid - not the vaccine.
The first source just measured declining antibodies, but the real picture about immunity is more complex than that. The second doesn't say what you think it says.
If getting the actual disease only results in 90 days of immunity, then will a vaccine do any better? Is there precident for immunity via vaccine being longer-lasting than immunity as a result of contracting the actual disease?
That’s why the vaccine needs two applications. With only a single application, you’d also only get 90 days.
Additionally, a lot of the additives in the vaccine are intended to make your immune system perceive it as much more of a threat (while a virus will try to be perceived as not a threat), increasing the priority your immune system gives the virus (and the duration it will be able to stay immune)
As far as I understand those who were infected and recovered are still encouraged to get the vaccine. I’m not sure what that does to their priority in the vaccination queue though.
I think the length of time recovery and vaccination confer are still not really nailed down
A medical professional I know had COVID in November and just got her second dose. Anecdotally, it doesn’t matter if you’ve had it or not for the purpose of the signup process.
We'll unlikely reach said number because over 50% of the population of the us is not interested in a vaccine because they do not view covid-19 as a disease much more risky than the flu.
Facing this reality, the policy will probably be once everyone who wants it has had a chance to get it, things will or should move towards normal.
The number of people interested is up to 66% now (https://www.google.com/amp/s/amp.cnn.com/cnn/2021/01/21/poli...), and I think there’s good reason to expect it to keep rising as the rollout continues. It does seem likely there’ll be an awkward in between period where we don’t have quite enough takeup but the vaccinated people demand to go clubbing, but I don’t expect it’ll be too large.
The people who don't get the vaccine aren't just hurting themselves. We need herd immunity for people who can't take it, or for whom it won't benefit.
There are definitely people who may not benefit as much from the vaccine because they are immuno-compromised for example.
The only reason not to take it is if your doctor tells you not to. Unless they've told us not to for medical reasons, we should take it if we can get it, ASAP.
And I think pressuring people to take it is appropriate, given that it's not just them at risk.
Apparently the post you're replying to is not very popular. But I think both yours and that post make valid points that don't even contradict each other. Because even if we pressure people to do the right thing, after all, this is presumably a free country and there seem to be plenty of people (quickly scanning this thread for percentage quotes, dangerously close to ruining the presumed herd immunity level) who will refuse - or neglect - to comply. But what can really be done about this?
Pressuring in form of awareness efforts will take probably years, and who knows how many deniers will even get it. I'm starting to read posts and "studies" about paying people off, which I think is insane - (1) the whole idea of people who want to fix this problem actually having to bribe via their taxes those people who refuse to accept reality, and (2) payoffs can simply be abused in a million ways - but whatever, say we all take one for the greater good. But then even a large-scale payoff effort will also take months if not years.
What else can you do to pressure people? Restrict their rights until they get a shot? Tell them their kids can't go to school until they show a QR proof of vaccine? Realistically, just how can you pressure people if you are not in North Korea? So then we're back to everyone on lockdown because of the stubborn few?
In Australia, there are daycare subsidies worth ~50% the cost, gated by kids getting vaccines or a doctors exemption.
That largely works pretty well at keeping the pool of deniers down to the true-believers; it turns out that many anti-vaxxers give up their beliefs when it becomes personally inconvenient to hold them.
If your normalize getting it done and exclude people who don't from opportunities, you incentivize people who want to participate, not just in receiving the benefits, but in participating in the group.
I think of it much the same way I think of driver's licenses. I believe if you are driving on your own private property you don't need one. But if you are using public roads and putting people at risk, there's an expectation of training and the ability to revoke permission if you harm others.
Don’t forget the collateral damage of vulnerable people that cannot take the vaccine for whatever reason. Australia just passed for ages 16 and up, no idea if people under that age with other conditions are SOL or if they’re allowed to bypass that restriction. Fortunately, the population here are generally pro-fax, I assume to the point where herd immunity is actually viable.
For large portion of the population, it isn't. 99.9+% for many demographics. I'm not interested in it personally, as one of my dad's coworkers got Bell's palsy from the vaccine. Given my age and risk profile, the vaccine isn't worth it.
> Nevermind the people who you infect and kill, you can’t be blamed for that, right?
This is a new standard. Even though the flu is very dangerous in small children, adults who mix with adults in work settings while infected with the flu have never been held to this standard. And since everyone might carry something that might be dangerous to someone under the right circumstances, I never wanted to go down the road of locking people up just in case someone somewhere may possibly be spared an infection.
Keep in mind that solitary confinement is an additional punishment for most inmates in most prisons in the world. Yet, that has been inflicted on people without so much of a second's thought to what the costs are.
So, by your standard, nevermind the kid who kills himself because he has now been put in solitary due to forces completely out of his control. Or, the grandmother who lives in another country who may be spared a SARS-Cov2 infection, but lost most of her mental faculties due to lack of contact with other human beings.
Do you think the only bad thing that can happen to someone is a SARS-Cov2 infection?
If not, they one must take into account how much of one bad thing one is willing to tolerate in return for a given reduction in some other bad thing. Because the probability of some bad thing happening to someone is 100%.
There's no evidence yet (that I'm aware of) which is why experts are very cautious against giving false hope.
But based on past vaccines for other viruses and the way they and the covid vaccines help your body be better prepared to fight the virus, it's a reasonable guess that they may well at least limit spread, perhaps even close to prevent it.
So you're right to point out that it's not a sure thing, but I (admittedly, not an expert, but basing on views of experts) also think it would be more surprising if the vaccines didn't slow spread at all, the bigger question will be to what extent (both with and without current protective tools like masks and social distancing).
Even if there is no reduced spread, reducing load on hospitals has got to be a good thing. That’s assuming the vaccine doesn’t increase spread (where I’m assuming a reduced likelihood of symptoms)..
why is it the the responsibility for low risk individuals to put their lives on hold indefinitely so that high risk individuals can live recklessly? the elderly and the immunocompromised were at risk long before covid and they will be at risk post covid too. i cannot stop boomers from being dumb and selfish and acting with utter disregard for their own safety and 10+ months operating with an excess of caution and doing everything right were rendered utterly meaningless because they got me sick.
If someone were to transmit covid to me and I ended up dying, I would not blame this person for my death, unless they had acted with malice and purposefully infected me by spitting in my drink when I wasnt looking
I don't infect and kill anything. I'm not a virus. What kind of demented logic is that?
My uncle got the vaccine, and then a week later his family comes down with Covid, including him. They did fine, but it's not a guaranteed thing.
This particular vaccine isn't even a vaccine in the traditional sense, where they give you an inhibited version of the virus and let your immune system work on it. It's an mRNA cellular protein booster that is supposed to help fight it. It's all pretty new.
The fact that it's mRNA isn't really relevant to how your body fights the virus, it's still the same mechanism.
The traditional way (as used by the Oxford/Astrazenica covid vaccine, and others) is to show the body what the virus looks like by giving it non-harmful bits of protein that look like the bit of the virus the immune system will need to recognise.
The mRNA ones (like Pfizer's or Moderna's) use mRNA code to tell your body to create those harmless proteins, and then the rest is the same - your immune system learns to recognise them, which is good because it will be more likely to recognise the real virus.
The mRNA technique is just moving the "create these harmless things" from the lab to inside the body. It doesn't change how your body fights the virus compared to traditional vaccine methods.
(mRNA vaccines have also been undergoing safety tests for years, these ones for covid are the first approved but not because previous/ongoing ones were shown to be unsafe.)
You might be right, I'm sure they have been studying them in the lab for years. But having already seen someone suffer from Bell's palsy as a direct result of the vaccine, I don't need that risk. Especially since people in my family who are genetically similar to me and of similar overall health have already contracted Covid and never got worse than a typical flu for any of them, and for several of them they never even got ill. Coupling that with the knowledge that for my age and demographic profile, I'm at no statistically significant risk, I choose to risk exposure to the virus without the mRNA vaccine. That's how it has to be.
Very sorry to hear about the person you know with Bell's Palsy, I wish them well and with some luck hopefully they'll recover from it and get back to normal.
However, there is not yet any evidence I've seen that the vaccine can cause Bell's Palsy. There's not conclusive evidence it can't, but the FDA says: "The observed frequency of reported Bell’s palsy in the vaccine group is consistent with the expected background rate in the general population."
(Please do correct me if I'm out of date and there's anything showing statistical significance, but I don't see anything new from a quick Google.)
When you vaccinate a lot of people, some of them will develop medical problems that would have developed regardless of the vaccine. It's not impossible you will be proven right once there is more data, but until then it is spreading misinformation to say that the vaccine did cause the problem.
The number I have seen quotes form Dr Fauci is 70-85%. However I have seen no studies so far that show that either of the vaccines used in the US slow down the spread of COVID, just that they prevent severe cases. Also neither has been tested in children under 16 which is obviously a large population.
That's single dose, so you gotta double it. And account for like 40% of the country that are not sure if the pandemic is real and/or if the vaccine is designed to have Bill Gates track them. And the fact that kids can't get it yet (and who knows when we will know), which would severely slow things down.
Right now we are production-constrained, and somewhat distribution constrained since every state is handling it differently. But soon enough we will be constrained by people's unwillingness to get vaccinated, and then things will get really fucking annoying.
The UK has something like the 4th most Covid-19 vaccinations per capita of any country in the world, and the gap between it and other western countries is quite big from what I recall. (All the countries with more are much smaller, meaning that they could achieve that with a much smaller vaccination program and fewer doses than would be necessary to do the same in other countries.)
A lot of Americans have already stopped complying with public health recommendations. Or they never put on a mask to begin with. It's like a teacher who tells a class to line up so they can be dismissed but someone doesn't go along and drags out the whole process.
One might reasonably believe that clearly defined exit criteria might boost compliance if chosen carefully with community input. I can see the other side of things. In my opinion we are doing a very poor job of meeting people’s needs.
People were only in this together for a few weeks in March and April. I can somewhat understand as losing one's job is losing almost everything in America. Our leaders frittered away two months of advance warning, provided contradictory advice on masks, and botched creating a test. Compare the United States with Korea which had their first confirmed case on the same day.
"Two weeks to slow the spread" while we build up hospital capacity has turned into nearly a year of not bothering with extra capacity. It doesn't surprise me people are fed up.
It takes years to train a nurse and a decade to train a physician. An indication of max capacity is when hospitals halt elective procedures. There are currently 130K people laid out in hospitals. We have mercifully just trended down from a third peak. Would you rather we get Italy's fate of mass casualty stage rationing?
Here in Chicago we built [0] and staffed [1] extra capacity, and then got rid of it a short time later when it went almost completely unused [2]. Despite early claims they could, they did not bring it back for the second wave this past fall [3].
There was no reason for us to stay as locked down as we have been.
You're talking about now, I'm talking about then. We had a ton of extra unused capacity and could have loosened restrictions back then, but didn't. If we had, then maybe people could have handled doing this longer, but we didn't and so people care less and less about following the restrictions.
Ok, so take a look at this data page from Germany, if you mess with the graphs a bit, you'll see new cases drop off around June, in time for summer holidays. Germany chose to reduce restrictions at that time. That's reasonable, right?
https://news.google.com/covid19/map?hl=en-IE&mid=%2Fm%2F0345...
All of these are having a bit more trouble with the second wave, Clearly something has changed about the nature of Covid. But you can see them weathering the first wave, and dealing with the second wave. You see how the number of cases drops off to near 0 during summer?
Take care: that Y axis is much larger than the other examples above.
On June 1 2020 there were still 22000 measured new cases on that day alone. Sure that's a slight drop from the 34000 cases on April 9. But that's not really safe to loosen restrictions, now is it?
(Now we do know that that's an aggregate and some individual states have done better. You can drill down to get that information.)
You continue to ignore the extra hospital capacity that is my entire point for here, but I'll just add - the cases started dropping Nov 16, days before the new restrictions went into place. If it was the new restrictions having an effect, they shouldn't have started dropping until somewhere around Dec 5.
I think it's safe to assume that they were probably at "Tier 2" prior to Nov 20?
Due to the way that Covid is stealthy, you don't see the effects of policy measures for 14 days or more. It's not very surprising that policy measures would lag behind the curves.
And I don't really see a problem with the extra hospital beds. This particular pandemic is really hard to manage. If someone accidentally prepares more hospital beds than they need, that's perfectly fine by me. That's a much better plan than not having enough.
Unless you think that protecting citizens from harm (foreign or domestic) is not a duty of the government, I guess they're doing as good a job as they can, given the circumstances. It's not pretty, but then again it can't be.
Wait, just to be sure. I just realized ... Would your idea have been to allow the extra hospital capacity to be filled up?
Eh, probably not.
You'd know that some people who are hospitalized also die.
Also; knowing the difficulty of trying to deal with an exponential curve, how would you be sure to cut off at just the right time, before people start dying in the streets?
Ok, no, that can't be it. I don't think people are monsters, so you're unlikely to be one :-) .
> Would your idea have been to allow the extra hospital capacity to be filled up?
Not completely filled, but yes, this is exactly what I've been saying. If we had allowed the extra capacity to get used, instead of getting rid of it, the lockdowns wouldn't have had to be as strict. Less strict lockdowns means less economic problems, which means we could sustain them longer.
Which gets right back to my original point: As it is now, people have ended up with more pressing concerns than the virus and so care less and less about following the lockdowns.
Also another quick aside, back on that original point - "two weeks to slow the spread"? Lockdowns were sold to us specifically on slowing the spread while we increased capacity, to deal with the increase in patients. There was always an understanding that as long as we don't go past that capacity, no extra lives would be saved, they'd just be spread over a longer period. That's why the original slogan was "two weeks" - it was what we needed to build the extra capacity, then we could stop the lockdowns as long as we kept masks/social distancing.
I don't know what you were sold, of course. But surely you agree that deliberately making/letting people get sick is obviously evil.
What could possibly be a more pressing concern than people's health?
Indeed in many countries the original restrictions were lifted or ameliorated after the first wave. However -just looking at the numbers- obviously something went terribly wrong in the United States overall, and authorities were not able to keep their promise.
This sucks terribly. It doesn't magically make it safe to not have restrictions, of course.
> What could possibly be a more pressing concern than people's health?
"Health" is far more encompassing than "don't get the virus". I'm also talking mental health and security (food and shelter), both of which have been badly affected by the lockdowns and lost jobs from the lockdowns.
> obviously something went terribly wrong in the United States overall
There's (at least) two things going on here, neither of which has to do with the response:
* The US is big. Half the country has a different climate than the other half, and all evidence is that SARS-CoV-2 is heavily seasonal. What you're seeing in the country graph is as it recedes in one set of states, it grows in another set. Check out the curves for southern states like Florida, Mississipi, or Arizona - their first wave doesn't start until the summer, after first wave in the northern states like Illinois have already ended. Add them together and you get the consistently high rates for the whole country.
* Too-high-cycle PCR positives without symptoms being counted as a "case". The WHO just changed their recommendations last week because PCR testing has been being misused (as people have complained about since at least last summer) to take into account the false positives and symptoms; if these new recommendations are actually followed, expect the case rate to plummet pretty rapidly (though perhaps not sharply as different states may adopt it at different times).
You might argue in this case they could have theoretically backed down restrictions to a lower level, once they saw that the lower level was already having an effect.
But in leadership, it's often good to stay a given course, if it is at all helpful. In this case, it is, You get back down to lower infection numbers faster, thus allowing people more freedoms again sooner.
I would rather that our leaders be honest from the start about what we’re facing and what they plan to do about it. I’m extraordinarily skeptical that trying to control public opinion by boiling the frog is effective.
Is it possible to create clearly defined criteria when there are such large error bars and so many unknowns? Throw in varying climates, urbanization levels and other factors and I don't think it's reasonable to pick an arbitrary point. Re-openings in most of the world have been staged anyway.
Hopefully the decisions will be data driven like they are now. When the number of new cases, positivity rates, and deaths in a given region fall below specific thresholds, the next phase of opening up happens in that region. Then those numbers start to increase, then restrictions start going back in place. The same as it has been since the start of this pandemic.
With those that are the most vulnerable (front-line workers, elderly and health compromised), hopefully the death rate will start to fall as they are getting the vaccine first. That is what I'm looking forward to.
I am not an expert at all, but I guess it really depends on the effect that "precautions" have on transmissibility, and therefore... probably in at least a few months, not before - assuming the vaccines protect from the new variants.
The US has cities with more people than New Zealand. Comparing it to Europe seems more fair because both have a mixture of policies between regions, more similar populations, neither is an island, and they're both economically developed.
The US was hit about as hard as most comparable western countries in temperate northern climates. New Zealand is an extreme outlier, in another hemisphere and with a completely different climate, so the comparison isn’t really fair.
What exactly is so difficult about wearing masks for Americans?
I'm an expat living in Thailand, which has an exceptionally low number of cases due to consistent mask use and social precautions.
Even if the vaccine reaches a level of saturation that is deemed safe, wearing a mask is a sane precaution that does not hurt you in any way and potentially saves lives of those unable to receive the vaccine.
Who cares if my action causes problems for anybody else, yeah Freedom FREEDOM!!!! I'm the most important person in the world!!! ME ME ME ME ME My rights!!!! Freedom, oh and anything else is ism.
swap in whatever ism is the flavour or the month, I have no idea what any of them mean, but they are all BAD!!!
Sorry... couldn't help myself. There is something disgusting about how people cry freedom as an excuse to take actions that place everybody they encounter at risk.
Ya once I’m vaccinated, I’m done. The health officials have lied “for the greater good” for too long. CDC lied saying masks are not useful when they wanted to conserve
I imagine they’ll lie again and say something like 70%. Screw the “vAcCiNe iSnT 100%”. Nothing is sure. But we gotta keep going w our lives
In a pragmatic, level headed world, we could stop wearing masks once everyone above the age of 50 or so is vaccinated, as the risk of death and hospitalization for under 50s is dramatically lower, to the point where death by anything else is significantly higher.
In the shrill world of the media, point-scoring politicians, and people that believe we live in some kind of movie world where we can save everyone from everything, probably when everyone is vaccinated.
Two points:
- Long covid also affects younger people (1-2%), so we might not want stop wearing masks until the case numberes have fallen to less than 5 per 100.000 per week.
- we might not want risking that the virus mutates, so we shouldn't use infections amoung the young to get back to normal.
Also if your media perception is shrill world then you might want to change your perceptions/media channels.
> so we might not want stop wearing masks until the case numberes have fallen to less than 5 per 100.000 per week. - we might not want risking that the virus mutates, so we shouldn't use infections amoung the young to get back to normal.
Which backs up my point about being pragmatic. 50% of the UK population are over 50 where COVID risks are dramatically higher. The likelihood of death or serious hospitalization for under 50s is much, much lower. 20-something men in the UK are much more likely to commit suicide, or die driving a car than dying from COVID, or having long-COVID (it's something like 100x more likely IIRC but I can't find a link right now).
> Also if your media perception is shrill world then you might want to change your perceptions/media channels.
I'm not sure what country you are in, but in the UK, at least, the closest to neutral reporting is the BBC, and only for its news bulletins. For everything else, Sky News, newspapers, and so on, the whole approach is just unrelentingly negative, and point scoring against the Government and its advisors.
Who's to say that we will ever reach that point? COVID-19 will be with us forever [1], which means that governments can forever point to it as a reason to push for increasingly oppressive restrictions. The economic meltdown resulting from these restrictions is pushing even the most capitalist countries much further onto the socialism spectrum than anyone could have imagined just a year ago. Some political parties view that as a positive outcome, regardless of how it was achieved.
So as long as COVID can be used as a way to achieve long-standing political goals, there will be absolutely no political will to relax the restrictions, even as infection rates start to fall as a result of vaccinations. It will take serious pushback by the populace - people making it clear that incumbent politicians will lose their next elections unless restrictions are relaxed - to return to any sense of normalcy in a reasonable period of time.
I wish I lived in your reality. Where somebody has a Plan and everything is going as it is supposed to. Unfortunately that is not true. The virus is real.
I'm not sure how you could interpret that comment as saying the virus "isn't real". Of course it's real. I also don't think it was "planned," nor did I imply that. But it's certainly being exploited for political ends.
My answer to that would garner yet more downvotes, which I am not interested in receiving. I already get auto-downvoted by several accounts on every comment I make.
I assume you know the answer to the question you asked, and were just being argumentative, because the answer is quite obvious. But in case you really wanted to know, instead of answering directly, I'll point you to a few resources:
1) "For authoritarian-minded leaders, the coronavirus crisis is offering a convenient pretext to silence critics and consolidate power. Censorship in China and elsewhere has fed the pandemic, helping to turn a potentially containable threat into a global calamity. The health crisis will inevitably subside, but autocratic governments’ dangerous expansion of power may be one of the pandemic’s most enduring legacies." - https://www.hrw.org/news/2020/04/03/how-authoritarians-are-e...
2) "The outbreak of Covid-19 and subsequent pandemic has led to an alarming uptick in authoritarian behavior by governments across the globe, who are using the crisis to silence critics, an open letter signed by more than 500 former world leaders and Nobel Laureates claims." - https://www.cnn.com/2020/06/25/europe/coronavirus-authoritar...
3) "...as the crisis goes on, some leaders could order restrictive measures that make public health sense at the peak of the crisis and then extend them in the hope of quashing dissent once the disease declines....A harbinger of what is to come may have appeared in Hungary, where Prime Minister Viktor Orban asked parliament on 21 March to indefinitely extend a state of emergency that prescribes five-year prison sentences for those disseminating false information or obstructing the state’s crisis response." - https://www.crisisgroup.org/global/sb4-covid-19-and-conflict...
How are we being pushed into socialism and what policies being pushed are socialist? I don't see businesses being made public, nor do I see workers gaining any control over business or economic decisions.
I said that we are being pushed onto the spectrum, not that we have become a socialist country. But COVID restrictions have forced millions of people out of work/business and into being entirely reliant on the government for money. When a substantial portion of the population is reliant on the government for money, the government must increase its own revenue, and it will come after those that still have an income for that money. Taxes will skyrocket, but that is unlikely to cover the shortfall, so we will also have to continue printing money at an increasing rate - devaluing our currency and the savings of those that are lucky enough to have any.
Ultimately, having vast swaths of the population reliant on the government for money, food, and healthcare, with oppressive taxes for those who are lucky enough to be employed/in business, and a currency that is rapidly being devalued, is a pretty significant step on the road to socialism.
What a terribly ignorant comment, but I suppose it is indicative of what HN has devolved into. 500 former world leaders and Nobel Laureates agree with me [1], but random Internet poster guy (along with all of the geniuses that downvoted my comments in this thread) thinks it’s out something straight out of Qanon. My source for that is undoubtedly one you implicitly trust...CNN. Not “Q”. Here is a direct quote from it:
”...the letter's chief warning is that countries with strong democratic traditions could use the pandemic to introduce extraordinary measures that in the long run become ordinary, doing permanent damage to global democracy...”
You, and those who think and act like you, really should educate yourselves before you criticize things you apparently know absolutely nothing about. You guys are turning the Internet into a toxic place where discussion of undeniable facts, from your own news sources and in this case brought to light by a collection of 500 of the world’s most credible people, are dismissed as wild conspiracy theories - simply because those facts might call into question the motives of politicians you blindly support.
I had a bit of a frustrating experience getting my elderly parents signed up for a jab today.
They are patients of a local hospital conglomerate. (I realize that’s typical in the States, Kaiser et al., but I’ve been living in Ontario, where you’re not wedded to some particular chain.) The hospital system said they’d notify patients who qualify, which both of my parents do, in spades. Dad was just in the ICU, during the pandemic, thought not for COVID.
Now, how did they choose to notify people? Well, how would you choose to notify elderly patients? A phone call, right? Perhaps a letter in the mail? Maybe a text?
Ha. No. They are apparently notifying people…through their patient portal app. No push notifications. No email notifications. The message just appears in your inbox, and it’s up to you to find it.
Which is, you know, less than optimal for the patients in these 1a and 1b vaccine groups. You know what a lot of elderly people aren’t great at? Constantly checking an app to see if they got a message.
Of course, for all I know, they may have other methods to contact people. But do they communicate those methods anywhere? No.
Ugh. I know. This is all complicated and rolling out at record speed. I get it. The logistics of this whole mess are horrifying. But just the teeniest bit of information and UX design here would got a long ways.
How can it be worse? Well, you can not have insurance, but you already knew that one. You can have an insurance company that's poorly integrated with providers, resulting in "edge cases" that somehow always involve you paying more. A lot more. Here's the one affecting me, though: insurance companies use pricing to ensure that my employer picks a new plan every year, which always has an extremely decrepit sign-up process every year, which no doubt shakes some fraction of the generally young and healthy workforce from going through it at all. It usually takes hours, even for someone of my technical aptitude, because you have to go on a scavenger hunt for the correct links, ID numbers, and codes.
It's not bad UX, it's brilliant UX, but the masters it servers are... not us.
> Here's the one affecting me: insurance companies use pricing to ensure that my employer picks a new plan every year, which always has an extremely decrepit sign-up process every year, which no doubt shakes some fraction of the workforce from going through it at all.
That's probably not the insurer’s intent, since it's in their interest to have the most people possible enrolled.
People who elect the benefit but don't complete the signup process are still enrolled, they just can't consume the services until they run the gauntlet, discouraging service use and increasing profit.
Under the ACA Medical Loss Ratio rule, insurers must refund premiums if they exceed a certain percentage of reimbursed costs across a plan (there's a couple different tiers with different limits.)
In order to maximize profits, they need maximum utilization, which takes completing the signup, not just idle premium payment.
Eh, I've seen accounting rules of that sort worked around with relative ease. It's not difficult to find ways to spend money that send value back your way, and even when you're in that position it's always the right move to ask for more. Budgeting incentives 101.
To be fair, communicating medical information through some channels is illegal due to privacy/security concerns. However I know that Kaiser in particular does actually email you to say "you have a message", even though it won't say what that message is.
When you're at the hospital, you might be able to pop by the administration office to make sure that the email they have for you is correct... you know, for when the next pandemic comes and you have this problem again.
I'm interested in how vaccinating a small number of people can make a big impact on the effects of the pandemic. The risk of death and severity rapidly increases with age. We also have a good idea of the kinds of preexisting conditions put you most at risk. We have already been targeting health care professionals (increases health care capacity) and people over 65 (the majority of the at-risk population).
If we are able to reduce the severe case rate by 10x or 100x, do we even need to reach herd immunity or would to be best just to remove all social distancing controls and let it burn itself out, knowing that the negative impact from those infections would be small enough to not put a strain on healthcare resources?
If the 65+ group made up 90% of the hospitalizations and they all have been vaccinated, do they know why are the hospitalization numbers down only 40%?
We know of a half dozen human coronaviruses that stay in circulation rather than burning themselves out, so there’s reason to worry this one wouldn’t either. The exact question is probably academic, because it won’t be politically feasible to maintain social distancing when severe cases are down 100x, but we’ll definitely want to keep vaccinating.
The Dutch have started burning their bicycles in protest. That's a pretty good sign we're at the end of the public's patience for this. The deaths are terrible, but you know what killed more people over the past year? Cigarettes. And they sell those at the grocery store.
This is unabashedly great news. For those debating if it is a sterilizing vaccine, if it’s perfect, what it means, etc, I point you to the following chart from Moderna’s trial:
Great news, 5% of the population already. That shows me how my home country - Germany, which was once saw as example on the fight against COVID-19 - still far behind. We only vaccinated 1.8% of our population. I wonder if the credits of a good rollout and access to such amount of vaccine will be given to the Trump administration as it should be?
Of course they won't be. The US press will just keep on pushing the narrative that the US was failing on vaccination compared to the rest of the world and it was all Trump's fault, regardless of the facts, just like they did with Covid-19 mass testing after the US started doing better than everyone else at that last spring sometime. That went on for almost a year until it finally helped get him kicked out of office like they'd hoped.
yes, well he lost the election, that's why he left, but I agree that probably his administration won't get credit on that. The BIAS is too high on the news.
It’s hilarious how by default the map includes all of Austria, but not even all of Germany (half of Schleswig-Holstein is missing in the default zoom/pan on first load).
1.8% is pretty good compared to the rest of the EU right? I'm still not sure why a lot of countries started so late or so slowly.
Still, like a lot of things, the last 20% is magnitudes harder then the first 20%. Finishing vaccination programs will come down to how well each government can educate their populist. I fear this is where America will fall down.
I believe in the end of the day, it will be directly or indirectly forced. Like, people who were not vaccinated will be fined, or later, detained if they are caught leaving their homes. I just see no other way around it, or pandemic never stops in most countries.
Not sure where you're from, but most Western countries have no legal basis to detain people leaving their homes just because they're not vaccinated. There might be some restrictions like air travel though.
even though I agree with you, The government has no business in saying who and how many people I invite to my home, or either who i meet in the Park. And here we are.
There's an issue here in defining how long a state of emergency can last. For most people, a few days (as for a natural disaster) is perfectly reasonable, and years on end is obvious abuse of power. We're just in between at the moment.
that would just make sense or be fair if everyone get access to the vaccine before those passports are enforced. Otherwise the 80+ years old people are going to have a lot of fun in an empty world :)
yes, well in Germany, the Federal Minister of Health said that "Vaccine won't be mandatory" but there were already some decisions to fire/punish employees (i.e Nurses and Soldiers) that refused to take the vaccine. That's remember me the famous saying: "Nobody has any intention of building a wall" (Walter Ulbricht)
Populism x Virtue Signal is the ideology battle from the century. The populists believe in the chip implant and the "Virtue signalist" believe that to focus on the "Elderly" is the only right thing to do. In the middle are we, 99% of the population, in home arrest.
IMO 1.8% is bad for a region that are responsible for the technology/production and distribution. Maybe it reflects how less influential EU became in the World geopolitics?
> Populism x Virtue Signal is the ideology battle from the century.
Nonsense. Populism is LITERALLY Virtue Signaling. They're the same thing. So if there's two teams, one identify with a different word for the same thing, you might as well just call them team red and team blue instead.
The actual ideological battle is between those who believe that the world is complex and that learning about the world is really hard work, but can be done through iterated improvement (i.e. people who have an education, not just on paper, but who can actually reason and critically think about the things they learn) and those who start from the assumption that they basically got it all figured out (the anti-intelectualists). This starts as a simple difference in attitude, but with time one of these becomes smarter and more knowledgeable, whereas the other stagnates.
America has ~330 million people. Let's assume the 18.7 Million was just in the month of january..not 100% acurate, but not 100% inaccurate.
That gives us a timeline of more than 1 year at current rate to vaccinate the entire US. Even vaccinating 70% the population will take roughly a year at current pace.
Not only is production still ramping up, but keep in mind the following:
1. As time goes on, more staff is trained and protocols are learned. Bugs are ironed out. Vaccinating people becomes faster overall.
2. All the high-impact vaccinations are done at the beginning. By the end of January, most western countries will be done vaccinating their highest-risk groups. This is the highest impact of all the vaccination phases because the high-risk groups represent the highest amount of hospital cases, so this will greatly reduce load on hospitals, which in turn will reduce transmissions in hospitals and free up healthcare personnel, and so on.
3. More vaccines are still being approved. The Pfizer vaccine is the one that is most in use right now, and it has logistical complexity attached due to its storage requirements. With more vaccines in play, this will become less of an issue making distribution easier outside of cities especially, and speeding up vaccinations overall.
There's good reasons to be positive about the vaccines right now. I do wish my country (Belgium) would focus all its efforts on it, because our current vaccination logistics are pathetic.
Yeah, in Q3 I was really hoping to be on an airplane this summer.
I realized in December or early January that due to the insane mismanagement it's going to ruin this summer too, and it'll likely be Q3 of this year before travel is really safe or reasonable again.
The US already has plenty of centralized health infrastructure (and did before Obama); this comment is a (partisan pot shot) red herring, and completely irrelevant to the vaccine distribution clusterfuck.
The issue is not lack of infrastructure, it's gross incompetence of the regional authorities who are responsible for distributing the vaccine.
If you thought the federal government sucked, wait until you see how bad the states are.
That’s what they said about the human genome project, back when it looked like it was going to take decades because of how slow the progress had been. (They finished ahead of schedule.)
I highly doubt we'll have an exponential curve for manufacturing supply.
Even a 2x increase is incredibly difficult. Just look at n95 manufacturing, a much easier problem to solve. We never saw exponential curve in its manufacturing.
Here is a interactive chart showing various nations [1]
Israel will be #1 by far. They have apparently paid $65/dose or something like that, far ahead of what others have paid, moreover, the dealing looks a little problematic. Obviously, it's worth far, far more than $65 a person, but it may not make too much sense to get into a vicious bidding war as it's unlikely to increase the rate of production and the surpluses would just be going into the hands of Parmacorps.
Misleading to say Israel is in the lead when the stats don't count the 4.5 million Palestinians living under their control, none of whom are being vaccinated.
Because the need for massive, acute production capacity for a specific variation of vaccine is short-lived.
What's the odds that we're going to have another pandemic in the next 10 years that has nRNA vaccine?
There's no need for massive production capacity other than during a global pandemic, and you probably don't know what you need, supply chains etc. until the time of production or thereabouts.
So - the money won't go into building out production capacity for something, when we don't know what that something is, it's constituent parts, or what technologies will be utilized.
The money printing that has been done because of COVID (that shows the economic damage) is many trillions of dollars, while the whole market cap of Moderna and BioNTech are in tens of billions.
The amount we're spending on productionizing vaccines is nothing compared to the damage the virus creates every day.
Businesses a failing every day, and when they go bankrupt they won't be able to come back.
I see...the RNA vaccine factory is useful though. Moderna announced already months ago that it is planning to have a flu vaccine next year. And for them changing the RNA sequence is really easy, so they can adapt their vaccine as the flu virus is mutating (just like what they are doing right now with coronavirus).
I agree. We need to start instituting temperature checks at all businesses and mandatory mobile phone contact tracing. This would help reduce crime as well.
So you’re advocating for persistent surveillance of people? This approach doesn’t seem effective. Reducing existing underlying health conditions (obesity), improving surge capacity for hospitals, and domestic production for critical supplies all seem like better places to start.
Does anyone know where I can find how many doses have been distributed to each state and how many are stockpiled federally or by the manufacturers? That’s the info I really can’t seem to find and it would be really interesting to see. Also would love to see production numbers day by day if possible. The simplistic estimates I keep seeing on places like CNN basically just take the current daily vaccination rate and use that as the rate for future projections which is obviously incorrect as production and distribution is ramping up.
This site is nice, but also it only shows the percentage of people who got a single dose, which is basically meaningless. We really should stop counting a dose as one vial and stop counting how many people got just one dose.
...or, at least halfway there (both Pfizer and Moderna vaccines require two doses). One dose is probably already somewhat useful, but how useful is not super-well characterized.
I saw a data plot from Pfizer's trial. Between 7 and 14 days after the first shot the number of infections falls off. Also a report from Israel says infections and hospitalizations fall 60% three weeks after the first shot.
Israel is definitely the place we'll see the first big impact (or at least we all really hope so). They are already well past 30% with the first shot. I was kind of nervous last week, when they were the leading nation in the world at getting vaccinated, and simultaneously shooting up to new record highs of new cases. But, this week we are just starting to see the first signs of a beneficial impact. This would suggest that you need something like 30% of population with one shot (depending on how many have already been infected, of course) to see a slowdown.
The U.S. is currently at 5%, and we're actually one of the countries furthest along.
At 30% with first shot they're probably half way there to effective herd immunity. One thing I read out of Israel was vaccinating the most venerable would bring the death rate down dramatically. Something like a 80/20 applies.
What I'm worried about is a surge in infections in the gap between population wide herd immunity and just most the venerable. As the death rate falls people will get really careless.
The confirmed cases in Israel is over 6% of the population, and the multiple of that which would include asymptomatic and others who just didn't get tested is unknown, but probably somewhere from 4-8. Even if it's as the low end of that range, you could already be halfway to herd immunity.
Of course, the ones getting vaccinated may often already have had it (whether they know it or not).
Since the death rate tends to lag the confirmed cases rate by a couple weeks, I think the deaths will still go up for a bit regardless of whether or not people get careless.
Can someone help me understand the difference between this and other vaccines? From what I know, the COVID-19 vaccine is only effective in reducing symptoms for those who get inoculated. Is it accurate to say this vaccine does not prevent infection or help develop an immunity? I just do not understand how vaccines work. Would love a (peer-reviewed) source or sources I could read to brush up.
This is not a political or bait post I really am looking for some signal in all the noise.
Vaccines never quite prevent infection. What they do is give the immune system a head start so they can overtake the infection early. Hopefully early enough to prevent symptoms, and ideally early enough to prevent transmission.
But just how early the immune system can win will depend on the strength on the immune reaction and the specifics of the virus. So for this specific one we don’t yet know whether it’s early enough to prevent subsequent transmission.
For example if transmission would require coughing and you never develop a cough, then there probably won’t be much transmission. But the potential for pre-symptomatic transmission suggests that it won’t be that simple, and while in theory this should reduce transmission it probably won’t eliminate it entirely.
As I recall from the news around the time the Pfizer vaccine was approved, the results from the people given the vaccine (vs. the placebo) was that it both reduced the rate of people who tested positive for the virus, AND reduced the severity of the symptoms to the point that the hospitalization rate was way down and the death rate was zero.
These are basically the same as the 'subunit' type of vaccine, with the difference being that your body produces the subunits directly through instructions in the mRNA that is in the vaccine. In this case the mRNA in the vaccine instructs your cells to create copies of the 'spike protein' portion of the SARS-CoV-2 virus that causes COVID-19. After being created by your own cells, these proteins enter the blood stream, trigger an immune response and ultimately immunity to viruses having that spike protein.
This is extremely targeted immunity vs. natural immunity generated by an infection, in which your body will create antibodies for all sorts of proteins in the virus. The broader resistance from natural immunity sounds good, and does have some benefit, but it also increases the risk of making your body react to its own tissues, creating an autoimmune condition. On the other hand, one potential downside of the mRNA vaccination is that if the virus mutates the spike protein sufficiently to resist the antibodies generated by the vaccine, you're back to square one.
> From what I know, the COVID-19 vaccine is only effective in reducing symptoms for those who get inoculated. Is it accurate to say this vaccine does not prevent infection or help develop an immunity?
As others have mentioned immunity does not mean 'zero infection', it simply means that your immune system is primed to stop the infection quickly by having antibodies for the spike protein.
There are a variety of COVID-19 vaccines either already approved or in the pipeline in various countries. Only some of them are mRNA vaccines, notably the one from Moderna. Others are based on older technology.
Cool, so the spike protein "factory" creates facsimiles of the actual SARS-CoV-2 spike protein, which then becomes a trigger to the immune system to create antibodies for that specific virus/spike protein combo.
The mRNA approach to vaccines seems to be a leaner, meaner, 2.0 version wherein instead of injecting a virus ut totum the vaccine-development-wizards have developed it to use just enough of the original virus code to trigger the immunological response, bolstering our defenses, and thereby increasing resistance to the thing "in the wild."
Would this apply to other coronaviruses, such as "common cold" type vaccinations? Were there specific discoveries in 2020 that will open the floodgates to better influenza protection? </rhetorical>
These types of responses are really helpful, and help me to get back into a rational framing of the subject - rather than fielding psychological noise from headlines and sub-informational news pieces.
It’s broader than that actually, this is a generalized protein factory.
This is how mRNA is created by the cells in your body to create the proteins needed to keep you alive (aka transcription): https://youtu.be/SMtWvDbfHLo
This is how mRNA is then used to create proteins, either from strands manufactured by your own cells, those coming from viruses that have infected your body, or from mRNA vaccines (aka translation): https://youtu.be/TfYf_rPWUdY
Not directly related, but here is an amazing video showing how HIV infection works, including parts you will now recognize from the above: https://vimeo.com/260291607
Well I guess that depends on what you mean by “true immunity”. If you mean not a single cellular infection, then that is ridiculous since true immunity doesn’t exists.
If instead you mean that you develop no symptoms, and cannot pass on the virus, then they indeed can and do (which is why r naught drops).
Now obviously if your “high viral load” is being literally bathed in viruses... then ok. But for many situations, typical viral load and even high viral load situations as seen in health care settings, many vaccines would qualify as giving large percentages of people “true immunity” in the sense of no symptoms and no viral shedding.
Another thing vaccines can do is prevent illnesses caused by toxins. In those cases antigens of toxic compounds generate antibodies to incapacitate a toxoids effect on the body, for example the tetanus and diphtheria vaccines or vaccines against rattlesnake venom.
These covid posts on hn are some of the most hostile threads I've seen on the internet. Between the intense emotions, conspiracy theories where people thinks they're constantly under attack, and various frustrations. Just don't take it personal. Or honestly dont bother with covid threads on this site. I'd treat them as read only and get your info elsewhere
Your body has two types of immune response, one called an innate immunity, which basically is programmed to attack certain types of pathogens at birth, and another an adaptive or acquired immunity. Vaccines target the adaptive immunity.
If we only had an innate immunity, viruses and other pathogens would learn to bypass it by hiding or disguising themselves in various ways. In order to counter this, our bodies constantly learn to recognize new pathogens. This is done by breaking down viruses into protein parts called antigens and creating antibodies that bind to those parts. Think of it like a lock and key.
Viruses typically have many proteins that can serve as these antigens on the surface of their cells. Many of these protein structures are actually used by the virus to bind to cells in our body and enter them.
Once antibodies to those antigens are being produced, they’re able to lock onto those surface structures and interfere with a viruses ability to function.
So a vaccine is simply a way to introduce those antigens and surface binding proteins in order to cause your body to generate an antibody immune response.
Another key component is that once your immune system creates antibodies, it “remembers” them through certain memory cells that are able to quickly produce the same antibody when needed at a later date.
Now all that sounds pretty simple, but the details get complicated, which is why vaccine effectiveness varies. Oftentimes certain types of viruses change their outer proteins so often, that a vaccine targeting one strain produces an immune memory that doesn’t work well with the next mutation.
Or other times the antibodies only bind to certain proteins that only partially interfere with virus infection. Or in some cases the way the vaccine is produced means that the antigens change subtly during the process making them less potent for good antibodies.
These new COVID vaccines are actually a method if introducing specific and accurate antigens to our immune system in a novel way. In this case it’s a bit of RNA that causes our cells to generate the antigen proteins themselves. It has the promise of being able to produce antigens of greater number and specificity than other methods. It’s basically using the same process as many viruses themselves (rna getting our cells to produce proteins) meaning our immune system is primed to take advantage and produce stronger immunity.
So the short answer is these vaccines are likely to produce strong and lasting immunity to the coronavirus they are targeting. What is unclear however is how fast this new strain of coronavirus will mutate into strains requiring more yearly shots to deal with changing antigen profiles (like the annual flu).
So the unknown is simply how this virus will evolve... if we’re lucky mutations that significantly change the surface antigens targeted by these vaccines will also mean the virus either becomes less contagious or less deadly.
If you’re truly interested I highly recommend this book on how the immune system works, full of excellent sources.
This I did not know - so basically there's a class of pathogens we have protections for at birth, and others we have to learn by exposure.
Antigens act as metadata of sorts from which our immune system can use to develop response mechanisms, do these antigens mean "permanent upgrade," in terms of our immune system recognizing it? (Yes, memory cells - cool!)
Just ordered a copy of the recommended book from my local library, thank you for the February reading list.
You got it! The memory cells seem to be able to last many decades through special cellular processes.
Hope you like the book. It’s a fascinating read. My favorite part is when he describes how the immune system is basically able to fuzz test for antibodies. It recombines and quickly mutates its own dna to generate way more antibody types than otherwise would be possible.
> From what I know, the COVID-19 vaccine is only effective in reducing symptoms for those who get inoculated. Is it accurate to say this vaccine does not prevent infection or help develop an immunity?
These statements are not accurate, but I think that there may be a misunderstanding with the discussion of whether the vaccine prevents symptomatic spreading.
First, to the second part of your statement, no vaccine really "prevents" infection. A vaccine primes the immune system to fight an infection, but the immune system typically only recognizes the attack once at least some cells have been infected and start producing more viruses.
However, being vaccinated typically means that your body will wipe out the virus before it has a chance to take hold and make you sick. But this doesn't mean it is just "reducing symptoms" the way, say, Sudafed reduces nasal congestion without attacking the cold -- being vaccinated really does mean that your body's defenses are armed to fight and destroy the virus the moment it invades. So it's completely wrong to say it simply "reduces symptoms."
What I think you're confusing this with is that scientists are saying that there is still a chance that you can become infected and become an asymptomatic spreader, even if you don't get sick.
The scientists aren't quite sure if this is the case or not, because it wasn't measured in the large vaccine trials. It's very likely that the vaccine at least reduces your ability to spread the virus, if not completely eliminates it, because that's the way most vaccines work. However, the reason the question is still unknown because certain respiratory diseases can still be spread after vaccination, because those viruses can sometimes replicate within the mucosal tissues in the nose, "hiding" from the body's main immune system.
As for the rest, I haven't really gotten a straight answer on the vaccine. Seems there are people who say it is the best thing since slice bread, and others who say it will be about as useful as the yearly flu vaccine. No one actually knows.
My Adblocker won’t let me load the submitted site. I wonder if it’s stats are better than Bloomberg’s?[0] Which shows US & global distribution, also claims over 22m Americans have been vaccinated
The Bloomberg number is _shots given_, so one person receiving two doses counts twice. The link above counts _number of people_ with at least one dose.
One thought: do we need herd immunity at all? Wait, hold off pushing the downvote button.
Why is this virus a problem? Not strictly because of deaths, although one would want to avoid unnecessary ones. It's due to the pressure on the healthcare system, because many people end up hospitalized, even though most of them recover (more on long COVID at the end of the post).
The vast majority of people ending up in hospitals are also belonging in the "at risk" population. To relieve pressure on the healthcare system, these must be vaccinated (along with healthcare workers). But once the most vulnerable and the most at risk of hospitalization are vaccinated, the pressure on the healthcare system should lower or cease for the most part (and the early data from Israel seem to indicate just that).
Of course, vaccination should continue (for those who want to get vaccinated), but with the risk of overwhelming hospitals gone completely, it would not be a problem. So society should reopen. And yes, in this case the virus will become endemic (it almost is already, save for a handful of places).
What about the others? Aside those who vaccinate, those recovered who did not have serious complications can go on like normal, like everyone else. According to data from Qatar[1] the risk of reinfection is low, and, most importantly, the vast majority of reinfections are asymptomatic (and asymptomatic people spread much less than symptomatic people, FTR[2]). In the context of the virus mutating towards (in the timespan of years, rather than months) completely escaping immunity, it is much better to rely on a combination of vaccination and natural immunity, so that subsequent, possible reinfections are not severe. That would also give time to adjust the vaccines if need be.
Unfortunately even throwing natural immunity along with vaccination is now a taboo topic, given how politicized the debate has become.
"What about long COVID?" some people may say. Well, the problem with long COVID is that, while it certainly exists, it is poorly characterized. Most studies lack a baseline before infection (or rely on self-reporting), so it is hard to determine what and for how long happens after an infection. Lastly, "regular" pneumonia can actually wreck someone for months or even a year, and some of these issues we're seeing may due to that: we're just seeing them at an increased rate because more people are experiencing that.
I think you're right. From a policy perspective, what is driving the shutdowns is the negative effects when healthcare is overloaded, and that healthcare overloading is a clear consequence of uncontrolled community spread.
If(as?) vaccination disrupts community spread, that should reduce reported cases and hospital occupancy. When those numbers are low, that will trigger relaxation of restrictions where I live (and I expect in other places as well).
I think there would still be a desire to vaccinate to herd immunity, but given the limited supply of vaccines, it would probably be best to prioritize vaccine use where there's community spread over building herd immunity in other areas.
> * Herd immunity numbers assume no ongoing vaccination -- they more or less say, "If life went back to normal, would the virus slow down or speed up?"
I'd say ongoing vaccination (after herd immunity is reached) is irrelevant to the herd immunity calculation. Is that what you meant? Though we'd obviously still need vaccinations as much of the world will not have herd immunity for a long time, if ever.
And certainly the percentage needed will differ whether we assume social distancing and travel restrictions are continued or not. Personally I hope we keep a lot of it, at least a long while more. I really hate catching flu's and colds.
> ongoing vaccination (after herd immunity is reached) is irrelevant to the herd immunity calculation. Is that what you meant? Though we'd obviously still need vaccinations
Yeah, exactly. Depending on other model factors (like ongoing vaccinations, relative mortalities, economic costs etc) the best time (and degree) to open up may be earlier or later than the technical herd immunity point.
To make an unfair argument: is 65% vaccination the end of WFH, or just when we should open up outdoor dining? If we vaccinate the youngest 65%, clearly we'd have different restrictions than if we'd vaccinated the eldest 65%. Etc.
> Personally I hope we keep a lot of it, at least a long while more. I really hate catching flu's and colds.
Are you blissfully unaware of the enormous mental health and developmental problems these measures are causing, or do you just rate those as less important than suffering an occasional mild illness while you eat DoorDash and watch Netflix?
"Eschew flamebait. Don't introduce flamewar topics unless you have something genuinely new to say. Avoid unrelated controversies and generic tangents."
"Please respond to the strongest plausible interpretation of what someone says, not a weaker one that's easier to criticize. Assume good faith."
Please follow those guidelines and all the other site guidelines. Comments like this just tip the ship on its side.
Don't miss the "a lot of it" part while you're at it. Because I wasn't actually thinking about fully maintaining travel restrictions either, apart from things like the better air filtering, and required masks. Though I do think they should continuing refusing people who are obviously ill. Perhaps this one will bug you nonetheless.
And before you retort again to pick at what I said and why you are justified in attacking me angrily about it, please reconsider the wonderful guideline regarding responding to the best interpretation of what someone said, rather than the easiest to attack. This is great advice I need to work on following better myself.
Personal attacks are not ok on HN, regardless of how wrong another comment is or you feel it is. If you wouldn't mind reviewing https://news.ycombinator.com/newsguidelines.html and sticking to the rules when posting here, we'd be grateful.
Your comment would be just fine without the first and last sentences.
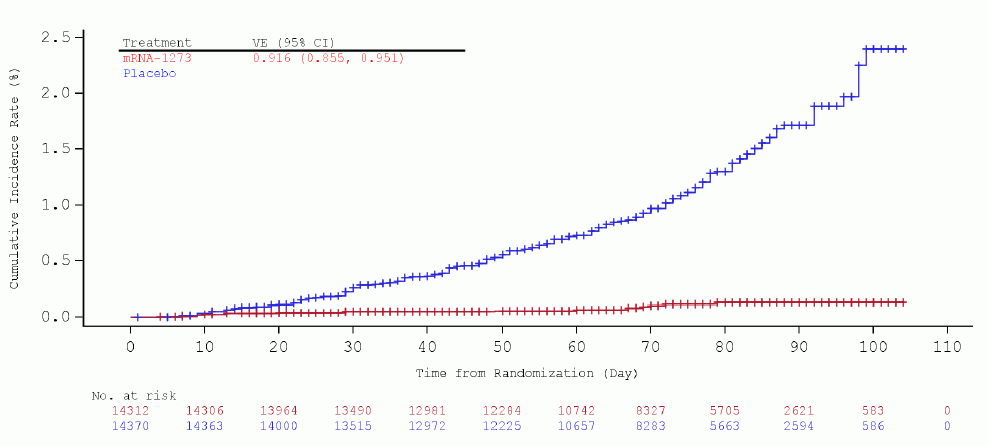{kind=link}